Speaking of motivated reasoning, last clause in pink box is a scientifically dubious interpretation.
Sisonke2 is a trial to give Sisonke1 participants (single-dosed J&J) another J&J dose as booster.
Sisonke2 is a trial to give Sisonke1 participants (single-dosed J&J) another J&J dose as booster.
https://twitter.com/MRCza/status/1463029057331810305
Gets worse after you click through. Really, no safety support? Trial organizers would actually withhold medical treatment if you have issues? I'm sure that's not what they meant, as it would be extremely unethical. So why use threatening words that imply it? 
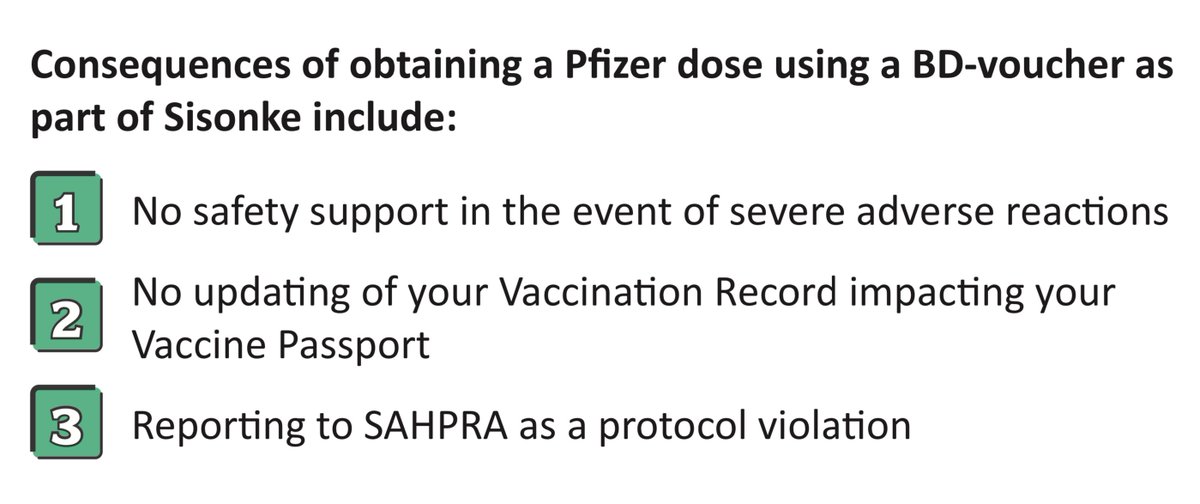
It's in reality a bit of a nonissue for safety, as there is *more* data in support of the safety of a Pfizer boost for J&J than of a J&J boost for J&J. So bringing it up is not scientifically valid either, and it seems to brought up only as a way to scare people away from Pfizer.
It's important that a trial of J&J booster would of course actually only dispense J&J booster, but the coercive language here does not seem like best practices for any clinical trial whatsoever.
• • •
Missing some Tweet in this thread? You can try to
force a refresh