
How much bullying is there NOW in surgery, and is the #OperateWithRespect project working?
In much anticipated news, the results of the @RACSurgeons 2021 Building Respect prevalence survey are out, as part of the very comprehensive Phase 2 evaluation.
A thread-
1/-
In much anticipated news, the results of the @RACSurgeons 2021 Building Respect prevalence survey are out, as part of the very comprehensive Phase 2 evaluation.
A thread-
1/-
The whole report is BIG- 185 pages. I'll bet this is the most substantial report into disrespectful behaviours by any specialty medical college anywhere worldwide. It indicates how seriously RACS takes the issue and makes me proud to be a Fellow. Link-
2/-
surgeons.org/-/media/Projec…
2/-
surgeons.org/-/media/Projec…
The prevalence survey results span pages 100-147 with the survey instrument spanning pages 148-185. This is all in the public domain and any College wishing to conduct similar research is welcome to access and build on it. Disrespect isn't just a surgical problem!
3/-
3/-
So, how much bullying, discrimination, and sexual harassment *is* there now in surgery after 6 years of #OperateWithRespect?
Well- more and less. A non- significant 2% increase in raw prevalence *but* measured over a shorter timeframe (12 months) *but* also...
4/-
Well- more and less. A non- significant 2% increase in raw prevalence *but* measured over a shorter timeframe (12 months) *but* also...
4/-

...an increase in awareness and knowledge of DBSH, which may mean behaviours normalised in 2015 are now seen for what they are. I know this myself- in the 2021 survey I ticked 'yes' for harassment based on sexist jokes, but I didn't in 2015...😬
#TheStandardYouWalkPast
5/-
#TheStandardYouWalkPast
5/-

So who is displaying the unacceptable behaviour?
Similar to 2015- males and surgical consultants. But it is improving, with some early evidence that DBSH from other groups are forming a greater proportion of aggressors. We *are* slowly getting our house in order.
6/-
Similar to 2015- males and surgical consultants. But it is improving, with some early evidence that DBSH from other groups are forming a greater proportion of aggressors. We *are* slowly getting our house in order.
6/-

In very heartening news for me and everyone else who has taken flak for speaking up immediately, delivering innumerable 'cup of coffee' conversations, and carefully considering when and how to escalate- the proportion of repeat episodes is significantly decreased. #SpeakUp!💪
7/-
7/-

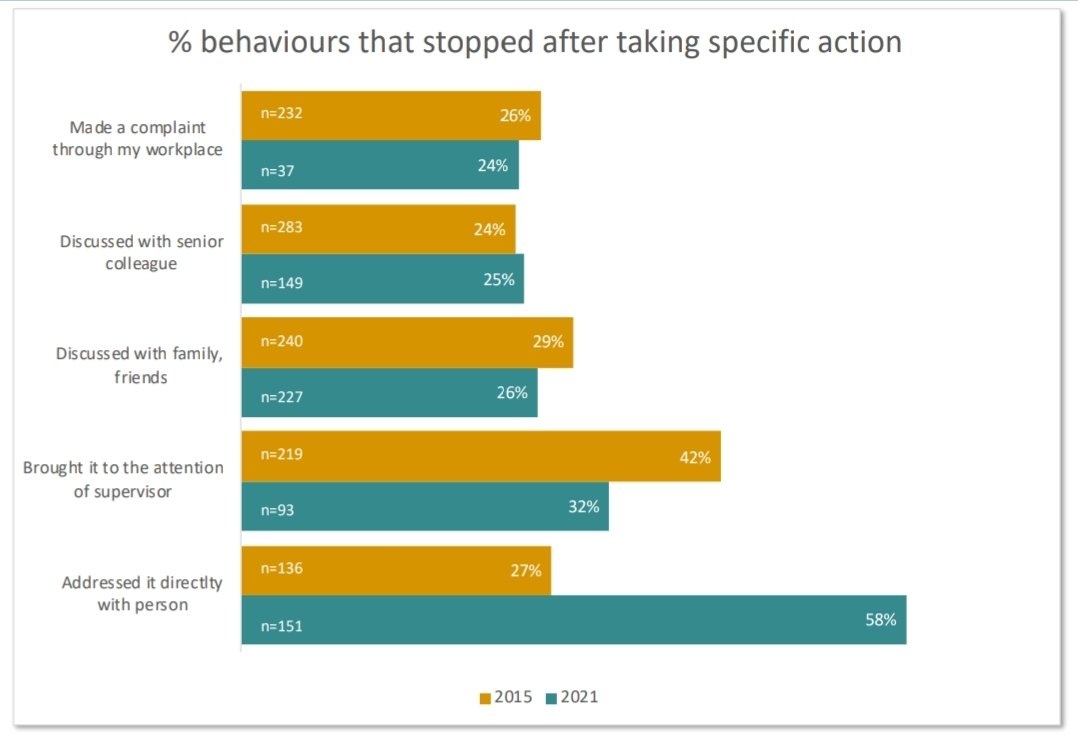
In more evidence that speaking up works, a far greater proportion in 2021 than 2015 found that disrespectful behaviours stopped after addressing it directly with the person.
8/-
8/-
We're not there yet though. 18% puff people who witnessed DBSH took no action and the factors that influenced their response, while showing a positive effect from the intensive education efforts around #OperateWithRespect, also show the negative effects of surgical culture.😔
9/-
9/-



So, where to from here?
There were many excellent suggestions from respondents👇.
And I've only given my take up to page 126. The qualitative data that follows is harrowing and uplifting in equal measure- another thread anon. In the meantime- #OperateWithRespect!💪
10/fin
There were many excellent suggestions from respondents👇.
And I've only given my take up to page 126. The qualitative data that follows is harrowing and uplifting in equal measure- another thread anon. In the meantime- #OperateWithRespect!💪
10/fin

• • •
Missing some Tweet in this thread? You can try to
force a refresh







