A few takeaways from this booster study from India’s perspective (we use adenovirus vector [AstraZeneca, Sputnik V] & inactivated vaccine)
They compared 2 groups of people: double vaccinated Pfizer and double vaccinated AstraZeneca.
A big menu of 3rd dose vaccines was used.
1/
They compared 2 groups of people: double vaccinated Pfizer and double vaccinated AstraZeneca.
A big menu of 3rd dose vaccines was used.
1/
https://twitter.com/RajeevJayadevan/status/1466749607312969730
The 3rd dose used were AstraZeneca, Pfizer, Moderna, Valneva (French inactivated vaccine), J&J, CureVac (mRNA), NovaVax (subunit, Spike protein).
They measured antibody level & T cell response after this dose, and compared between various combinations. See paper for graphs.
2/
They measured antibody level & T cell response after this dose, and compared between various combinations. See paper for graphs.
2/
The first thing we must remember is that antibody level is not an exact correlate of how much protection is achieved.
In other words, if “double” the antibody level is produced by a particular vaccine, it does not mean that symptomatic infection rate will be “cut in half”.
3/
In other words, if “double” the antibody level is produced by a particular vaccine, it does not mean that symptomatic infection rate will be “cut in half”.
3/
However, it is known that a very high level of overall antibody correlates with a lower chance of picking up an infection.
The exact level for an INDIVIDUAL person to “be protected” has never been defined because of tremendous variation between individual immune responses.
4/
The exact level for an INDIVIDUAL person to “be protected” has never been defined because of tremendous variation between individual immune responses.
4/
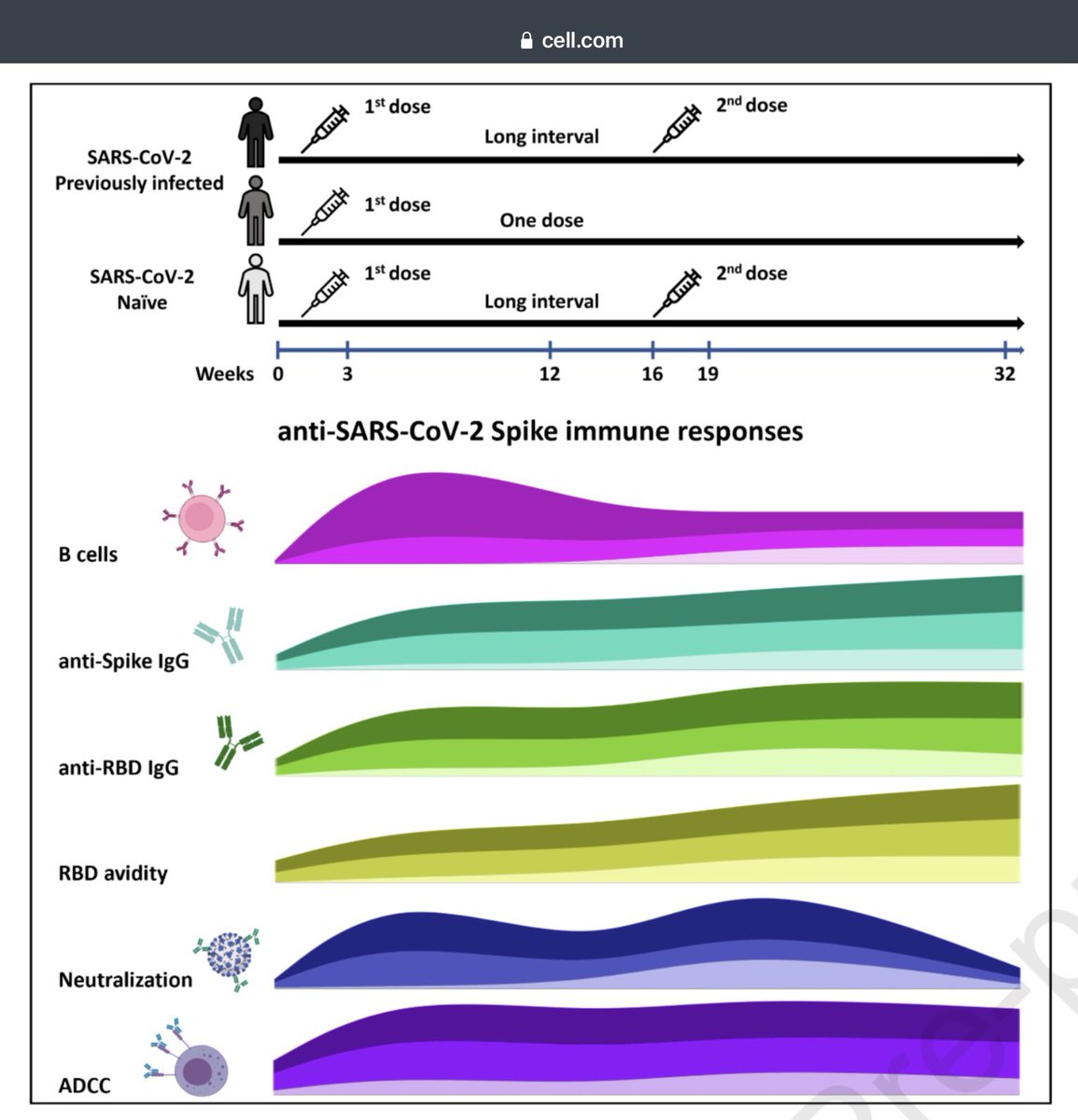
The distinction is less clear for T immunity.
It is known that both mRNA and adenovirus vaccines elicit T cell immunity which is long-lasting, manifest as consistent protection against severe disease and hospitalisation. This has not declined.
5/
It is known that both mRNA and adenovirus vaccines elicit T cell immunity which is long-lasting, manifest as consistent protection against severe disease and hospitalisation. This has not declined.
5/
T cells are elicited by day 10 of the first dose. Many of the earlier fighters belonging to the CD4 (T helper) and CD8 (T cytotoxic) genre remain in the tissues (e.g. lungs) and elsewhere as memory cells, vigilant against any future attack by the same pathogen.
6/
6/
It is unclear how to quantify the T cell response; evidence of their protection against severe disease is largely circumstantial.
Remember that lab studies are done on peripheral circulating lymphocytes- which need not necessarily represent what is happening in the tissues.
7/
Remember that lab studies are done on peripheral circulating lymphocytes- which need not necessarily represent what is happening in the tissues.
7/
Thus, it will be impossible to quantify the body’s T cell response after a vaccine dose. It is believed that T cell immunity is achieved early during the course of vaccination.
The epitopes these T cells recognise are numerous; many are impossible for the virus to alter.
8/
The epitopes these T cells recognise are numerous; many are impossible for the virus to alter.
8/
This property of T cell immunity is the reason why it is said that current vaccines are able to protect long term against severe disease caused even by variants.
Even if mutations occur, the majority of T cell epitotes are not altered.
8/
Even if mutations occur, the majority of T cell epitotes are not altered.
8/
With that introduction, some of the interesting findings of this paper can be summarised as:
1. For those who received 2 doses of Astrazeneca, taking a 3rd dose AZ generated only a slight increase in antibodies (GMT ratio 1.8), while there was no increase in T cell response.
9/
1. For those who received 2 doses of Astrazeneca, taking a 3rd dose AZ generated only a slight increase in antibodies (GMT ratio 1.8), while there was no increase in T cell response.
9/
2. For those who took two doses of Astrazeneca, using an inactivated virus vaccine as a third dose produced the smallest rise in antibody level among all the vaccines used. See below. There was no cellular immunity response.
10/
10/
3. mRNA vaccine generated the highest antibody levels when used as 3rd dose, among 2-dose AstraZeneca recipients.
The GMT ratio was ~15 (Pfizer) & 30 (Moderna) (compared to 3, 3.6 for AstraZeneca & 2.1, 2.3 for Inactivated VLA used as 3rd dose)
A higher ratio = more Ab’s.
11/
The GMT ratio was ~15 (Pfizer) & 30 (Moderna) (compared to 3, 3.6 for AstraZeneca & 2.1, 2.3 for Inactivated VLA used as 3rd dose)
A higher ratio = more Ab’s.
11/
4. Notably, neither AstraZeneca nor inactivated vaccine (Valneva) generated significant cellular immune response when used as 3rd dose in people who had received either AstraZeneca or Pfizer as their primary course.
12/
12/
In summary, this paper looks as how the measurable parts of our immune response respond to a 3rd dose of a menu of assorted vaccines, among those who received either AstraZeneca or Pfizer as primary 2 dose course.
This study is not a measure of 3rd dose effectiveness.
13/
This study is not a measure of 3rd dose effectiveness.
13/
This study adds to our knowledge about 3rd dose.
However the real test of effectiveness will be a long term follow up of similar groups of people who received different vaccine combinations, comparing how many of them (%) got severe disease over a period of time.
14/
However the real test of effectiveness will be a long term follow up of similar groups of people who received different vaccine combinations, comparing how many of them (%) got severe disease over a period of time.
14/
Observational studies are prone to multiple confounding factors which can lead to erroneous conclusions. These factors maybe overt or hidden, but can influence the conclusions.
Besides, several unvaccinated individuals would have picked up immunity from natural infection.
15/
Besides, several unvaccinated individuals would have picked up immunity from natural infection.
15/
Thus, comparing groups will not be a measure of vaccine effectiveness anymore, as there is no “100% unvaccinated control group” anymore, now that 2 years have passed.
We will, instead, be comparing people with varying combinations of infection, vaccination & boosters.
16/
We will, instead, be comparing people with varying combinations of infection, vaccination & boosters.
16/
@threadreaderapp please unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh