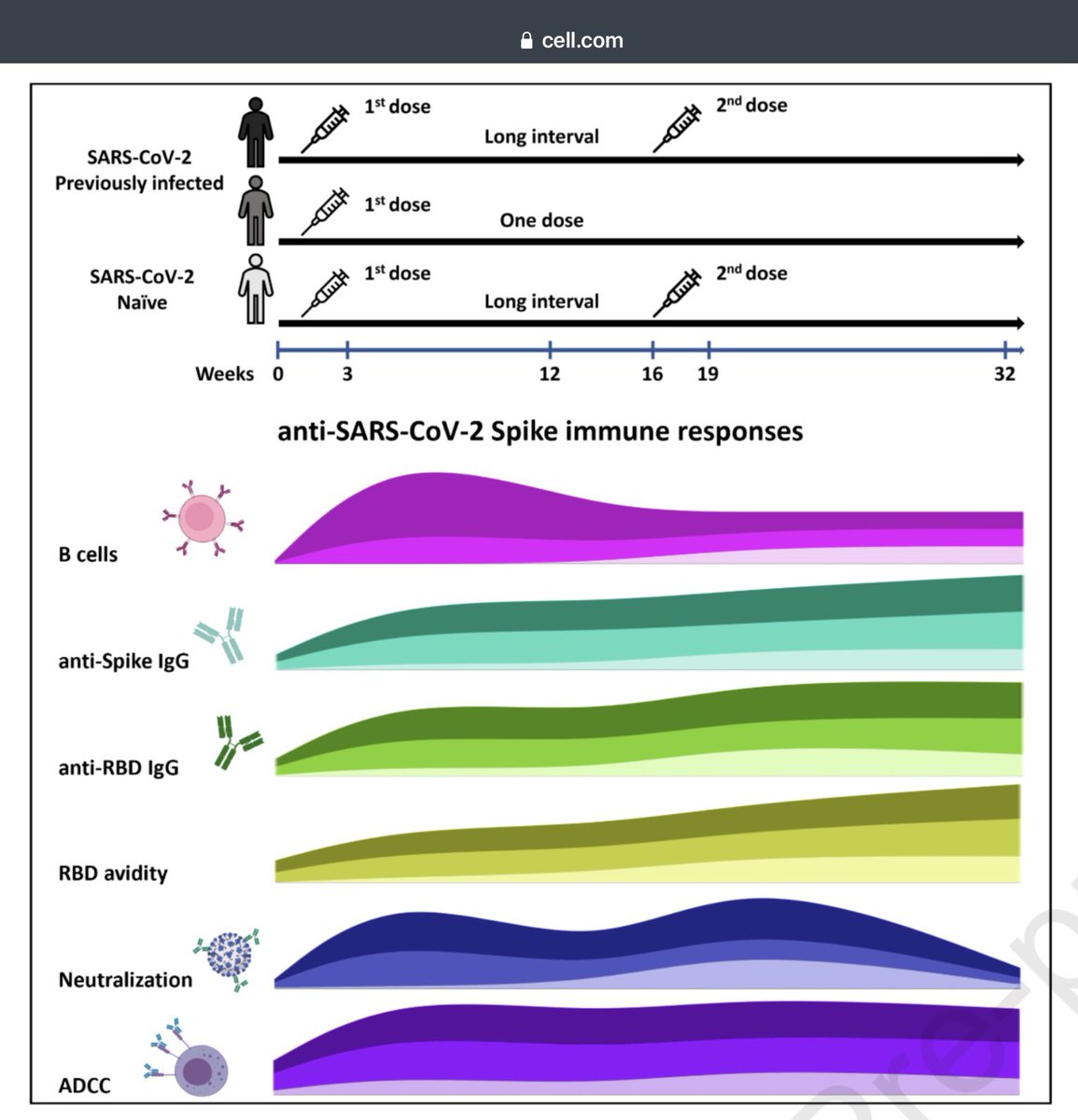
🔹Longer 4 month interval between doses generated stronger immune response (mRNA, humoral) than 1 month (16 vs. 4 weeks)
This ~explains the quick waning in nations that used short gap
🔹1 dose might be enough for those who had prior infection (2nd dose did not add much)
1/
This ~explains the quick waning in nations that used short gap
🔹1 dose might be enough for those who had prior infection (2nd dose did not add much)
1/
The study strengthens the original concepts that:
1. Single dose might suffice for those with prior infection
2. Vaccination for COVID-19 is basically a 2-step process, with a 3rd encounter not adding anything substantial. (The “booster dose” might have served as 2nd dose)
2/
1. Single dose might suffice for those with prior infection
2. Vaccination for COVID-19 is basically a 2-step process, with a 3rd encounter not adding anything substantial. (The “booster dose” might have served as 2nd dose)
2/
In other words, the first 2 doses of mRNA vaccine, taken “too close together” (3-4 weeks), might have been interpreted by the body as a SINGLE dose.
That will explain why the 3rd mRNA dose generated substantial rise in antibody level afterwards, during the booster campaign.
3/
That will explain why the 3rd mRNA dose generated substantial rise in antibody level afterwards, during the booster campaign.
3/
Note that the US used a 3 week gap for Pfizer vaccine; this was based on the original trials. This gap now seems to have been TOO SHORT to generate an optimal immune response.
This study used a 16 week gap (~4 months) and finds a remarkable improvement over the 4 week gap.
4/
This study used a 16 week gap (~4 months) and finds a remarkable improvement over the 4 week gap.
4/
The study also shows clearly that a second dose does not ADD to the immune response in someone with prior infection.
Previous studies had shown that cellular immunity also does not further increase after the 1st dose in these individuals.
(References in the Cell paper)
5/
Previous studies had shown that cellular immunity also does not further increase after the 1st dose in these individuals.
(References in the Cell paper)
5/
The study also shows “natural immunity” boosted by 1 vaccine dose declines at a slower rate than 2-dose vaccination (naive) - even after using the longer gap.
This suggests that the best immune protection is when a single dose vaccine is given to someone with past infection.
6/
This suggests that the best immune protection is when a single dose vaccine is given to someone with past infection.
6/
The authors write:
“The strong humoral response seen with this extended schedule is longer-lasting than immune responses following the authorized schedule, the need of a 3rd dose might be delayed and this could have significant implications regarding control of COVID-19”
7/7
“The strong humoral response seen with this extended schedule is longer-lasting than immune responses following the authorized schedule, the need of a 3rd dose might be delayed and this could have significant implications regarding control of COVID-19”
7/7
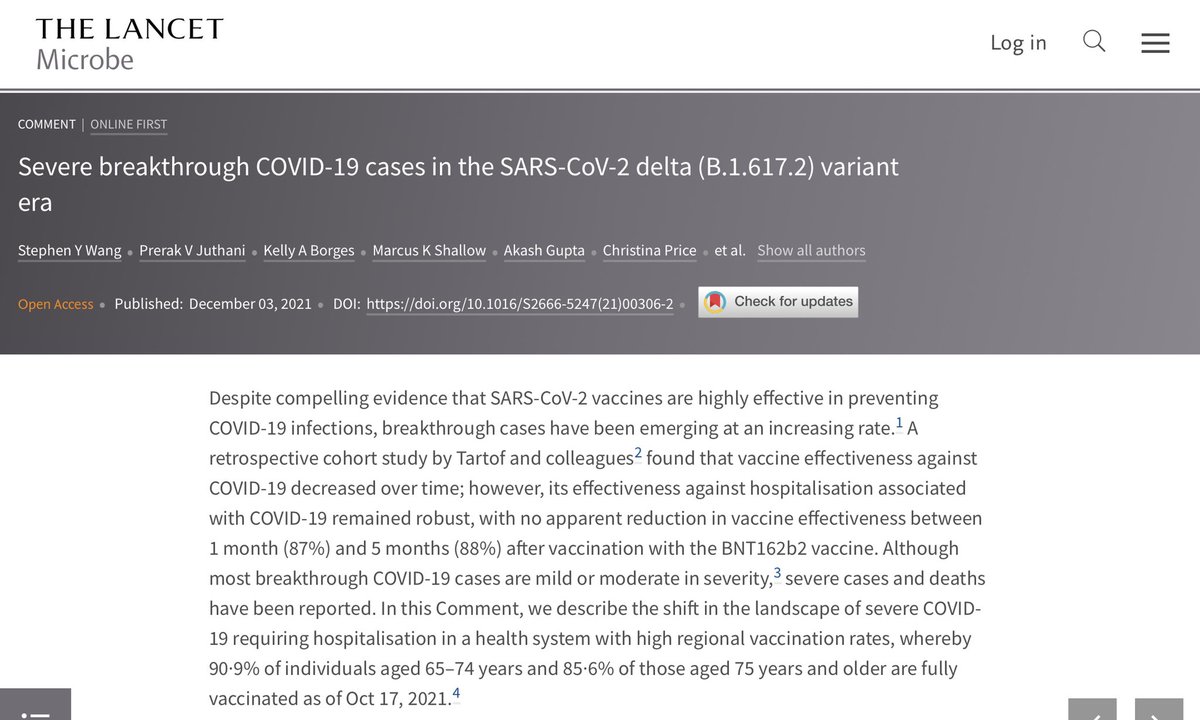
Link to Cell paper described in my thread above👆
cell.com/action/showPdf…
cell.com/action/showPdf…
• • •
Missing some Tweet in this thread? You can try to
force a refresh