The big picture on Omicron
Early studies now out comparing Omicron and Delta.
One liner: All is not lost; hybrid immunity performs the best.
This work is from @sigallab Sweden where they checked neutralisation of omicron VS delta VS old virus using serum from 34 people
1/16
Early studies now out comparing Omicron and Delta.
One liner: All is not lost; hybrid immunity performs the best.
This work is from @sigallab Sweden where they checked neutralisation of omicron VS delta VS old virus using serum from 34 people
1/16
https://twitter.com/sigallab/status/1468325162860826634
They find what is already known: that people respond differently to the infection.
That is, there is substantial variation in the profile of immune response between individuals.
Which means: we can’t generalise for one person. That is one thing we need to understand.
2/
That is, there is substantial variation in the profile of immune response between individuals.
Which means: we can’t generalise for one person. That is one thing we need to understand.
2/
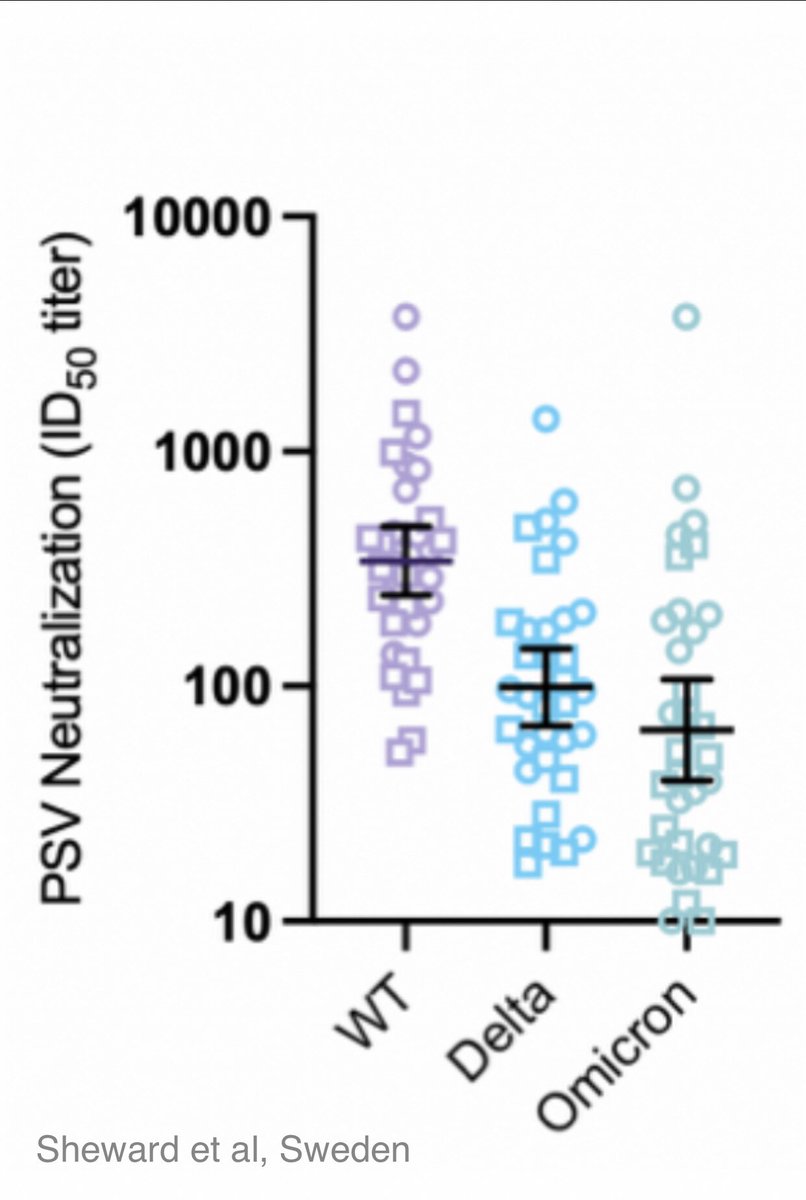
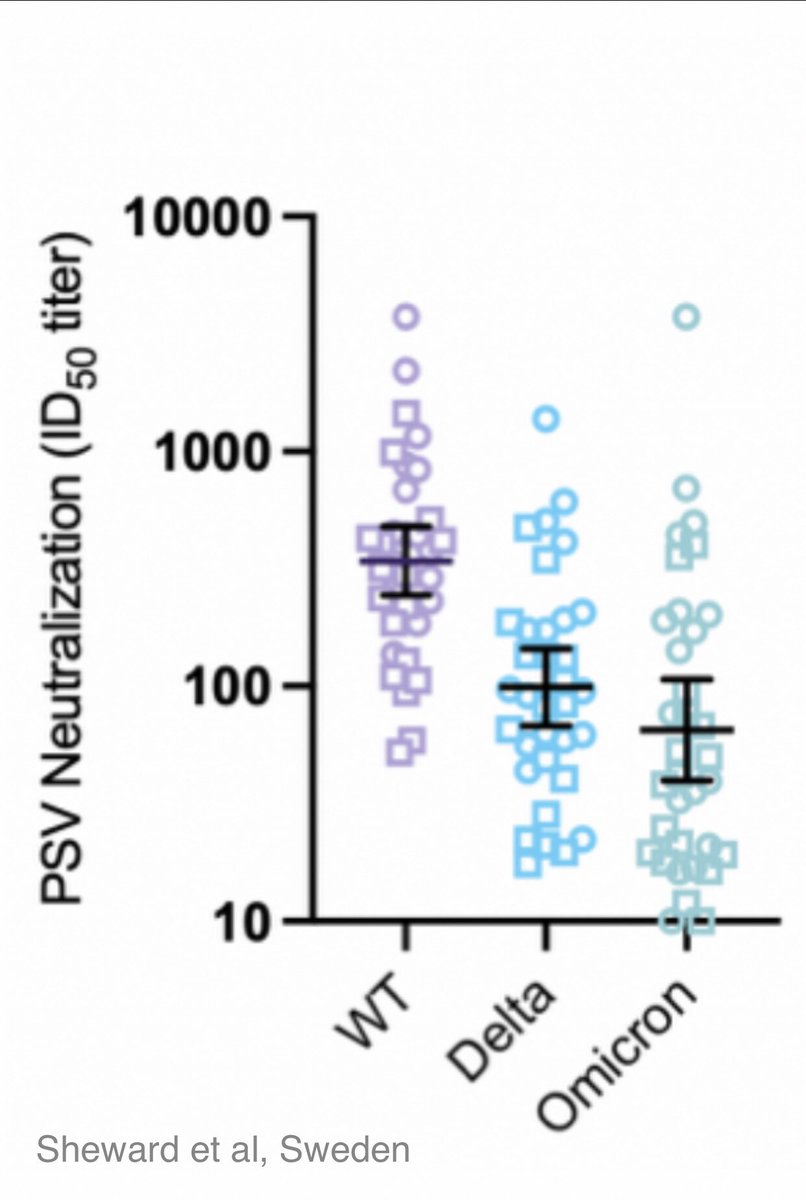
This graph shows all 34 people’s neutralising values
In plain English it means how did each of their serum (sera) did against: 1. Old virus
2. Delta
3. Omicron
The y axis is pseudovirus neutralisation titer. Higher value means the sample is effective at higher dilution.
3/
In plain English it means how did each of their serum (sera) did against: 1. Old virus
2. Delta
3. Omicron
The y axis is pseudovirus neutralisation titer. Higher value means the sample is effective at higher dilution.
3/
Obviously we want the serum to contain as much antibodies as possible, so that even when diluted many times over, it retains its ability to neutralise virus (that means, clog up its spike RBD and block it from entering the lab cells)
Which means higher value = more “power”
4/
Which means higher value = more “power”
4/
(Personally I would want to be among the top dots in that graph)
Now when we look at the 3 variants, we can see the relative difference between the three.
There is a trend towards the serum samples being less effective against Omicron, but we see it is not a “total loss”.
5/
Now when we look at the 3 variants, we can see the relative difference between the three.
There is a trend towards the serum samples being less effective against Omicron, but we see it is not a “total loss”.
5/
As viruses evolve, this can be expected. But that doesn’t mean the bottom dots “are all going to die”.
It simply means that there is evidence of the virus adapting to escape the antibodies to some extent. And that is so variable between people.
6/
It simply means that there is evidence of the virus adapting to escape the antibodies to some extent. And that is so variable between people.
6/
When we read scary headlines and tweets screaming “40 fold drop!!!” please keep this graph in mind.
The serum they used came from blood donors (recently collected, presumed vaccinated or infected, not specified) and healthcare workers (infected and vaccinated)
7/
The serum they used came from blood donors (recently collected, presumed vaccinated or infected, not specified) and healthcare workers (infected and vaccinated)
7/
As I mentioned, in this study they tested antibodies. They did that against “pseudovirus*” that is another virus where they inserted the spike protein of the omicron variant (it is less dangerous to do these experiments than with the real virus)
(Lentivirus pseudotype assay)
8/
(Lentivirus pseudotype assay)
8/
They did this so that they could study just what the spike protein behaved like. When serum was added, the antibodies clogged up the RBD and the virus failed to enter lab (tissue) cells.
They measured this preventive ability of serum, and the titer is expressed on y axis.
9/
They measured this preventive ability of serum, and the titer is expressed on y axis.
9/
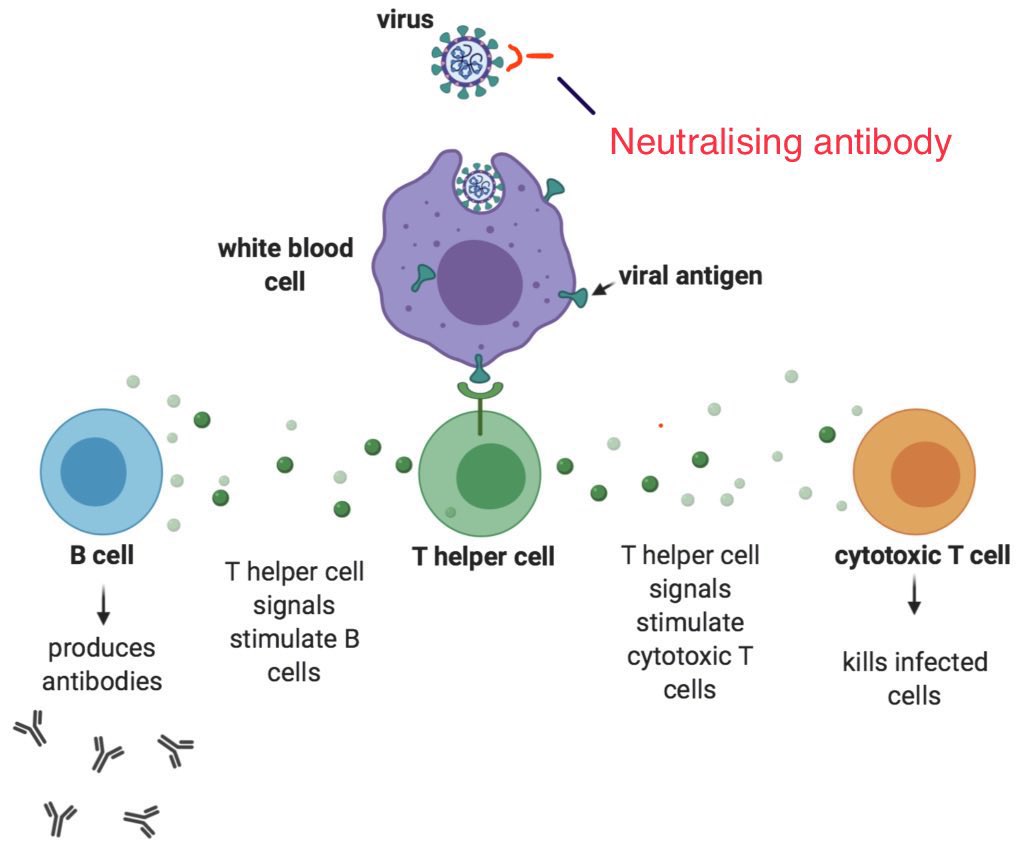
In summary it means that we have the ability to fight and win against Omicron. Early indications are that hybrid immunity (previous infection) followed by vaccination gives the best deal.
Also remember that immunity is a multiplayer game; here we just looked at a fragment.
10/
Also remember that immunity is a multiplayer game; here we just looked at a fragment.
10/
I would caution people from extrapolating “x-fold reduction in neutralising titres” into “x-fold reduction in total immunity”. Such an interpretation is not scientific, for the reasons explained.
T cell studies are under way. More papers awaited. There will be variations.
11/
T cell studies are under way. More papers awaited. There will be variations.
11/
At the end of the day, what we see in practice will tell the truth, and that will take more time.
The human immune system simultaneously involves multiple interconnected departments.
It is impossible to measure everything in the lab; not all components are even known.
12/12
The human immune system simultaneously involves multiple interconnected departments.
It is impossible to measure everything in the lab; not all components are even known.
12/12
Please unroll @threadreaderapp
@threadreaderapp please unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh