#IssaTweetorials
What is the mechanism of aberrant conduction?
1/9
“Aberration” describes transient bundle branch block (BBB) and does not include persistent QRS abnormalities caused by persistent BBB, preexcitation, or the effect of drugs.
#EPeeps #CardioTwitter #ECG
What is the mechanism of aberrant conduction?
1/9
“Aberration” describes transient bundle branch block (BBB) and does not include persistent QRS abnormalities caused by persistent BBB, preexcitation, or the effect of drugs.
#EPeeps #CardioTwitter #ECG

2/9
Acceleration-dependent BBB (aka “phase 3 block” or “voltage-dependent block”) occurs when an impulse arrives at tissues that are still refractory due to incomplete repolarization (during phase 3 of the action potential [AP]).
Acceleration-dependent BBB (aka “phase 3 block” or “voltage-dependent block”) occurs when an impulse arrives at tissues that are still refractory due to incomplete repolarization (during phase 3 of the action potential [AP]).

3/9
Aberration secondary to phase 3 block tends to be in the form of RBBB when premature excitation (and Ashman phenomenon) occurs during normal baseline heart rates and in the form of LBBB when it occurs during fast heart rates.
Aberration secondary to phase 3 block tends to be in the form of RBBB when premature excitation (and Ashman phenomenon) occurs during normal baseline heart rates and in the form of LBBB when it occurs during fast heart rates.

4/9
Phase 3 block constitutes the physiological explanation of several phenomena:
(1) aberration caused by premature excitation.
(2) Ashman phenomenon.
(3) acceleration-dependent aberration.
Phase 3 block constitutes the physiological explanation of several phenomena:
(1) aberration caused by premature excitation.
(2) Ashman phenomenon.
(3) acceleration-dependent aberration.



5/9
Pathologic vs physiologic phase 3 block
Acceleration-dependent aberration is a marker of a diseased HPS when it:
(1) occurs at relatively slow heart rates (<70 bpm).
(2) displays LBBB.
(3) appears with gradual acceleration of the heart rate.
Pathologic vs physiologic phase 3 block
Acceleration-dependent aberration is a marker of a diseased HPS when it:
(1) occurs at relatively slow heart rates (<70 bpm).
(2) displays LBBB.
(3) appears with gradual acceleration of the heart rate.

6/9
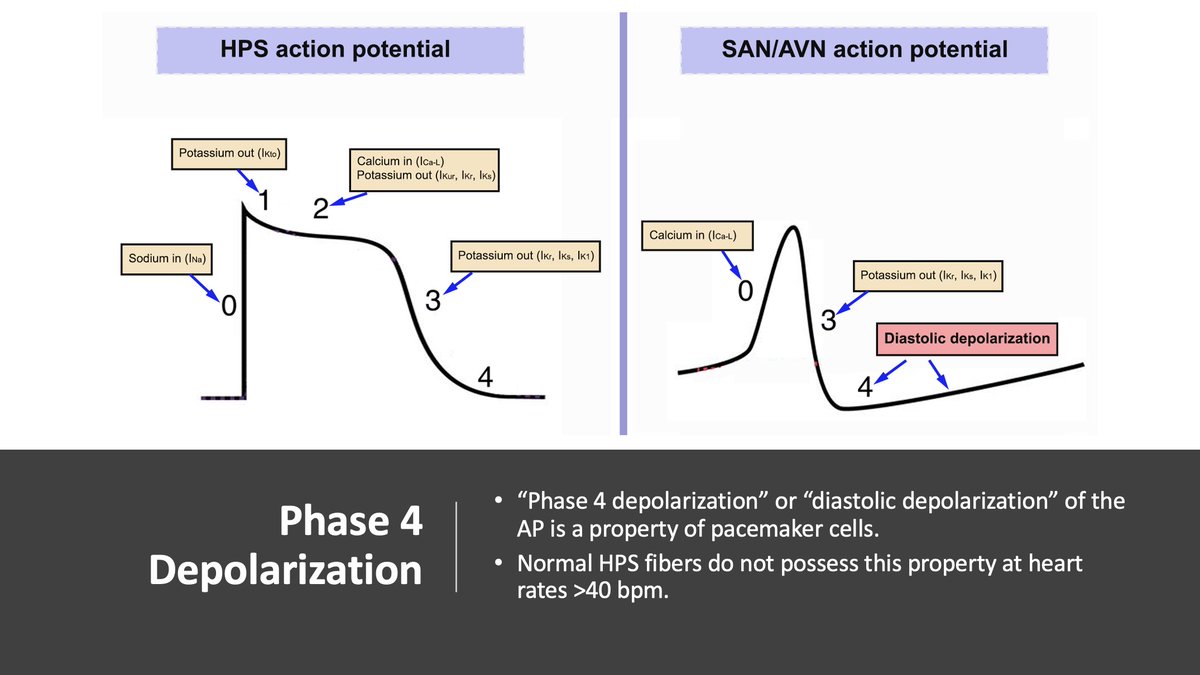
Pause-dependent block (aka “phase 4 block” or “bradycardia-dependent block”) occurs when conduction of an impulse is blocked in tissues well after their normal refractory periods have ended.
Pause-dependent block (aka “phase 4 block” or “bradycardia-dependent block”) occurs when conduction of an impulse is blocked in tissues well after their normal refractory periods have ended.
7/9
“Pause-dependent” or “bradycardia-dependent” block is caused by “phase 4 block.” Long intervals between activations allow for spontaneous depolarization and inactivation of Na+ channels & impaired conduction. Other proposed mechanisms include "source-to-sink mismatch".
“Pause-dependent” or “bradycardia-dependent” block is caused by “phase 4 block.” Long intervals between activations allow for spontaneous depolarization and inactivation of Na+ channels & impaired conduction. Other proposed mechanisms include "source-to-sink mismatch".

8/9
Phase 4 block often follows a delay caused by a compensatory pause after a PAC or PVC, spontaneous slowing of the sinus rate, or overdrive suppression of sinus rhythm upon termination of a fast supraventricular rhythm.
Phase 4 block often follows a delay caused by a compensatory pause after a PAC or PVC, spontaneous slowing of the sinus rate, or overdrive suppression of sinus rhythm upon termination of a fast supraventricular rhythm.


9/9
Concealed transseptal conduction underlies aberration in several situations:
1) Perpetuation of aberrant conduction during tachyarrhythmias.
2) Unexpected persistence of acceleration-dependent aberration.
3) Alternation of aberration during atrial bigeminal rhythm.
Concealed transseptal conduction underlies aberration in several situations:
1) Perpetuation of aberrant conduction during tachyarrhythmias.
2) Unexpected persistence of acceleration-dependent aberration.
3) Alternation of aberration during atrial bigeminal rhythm.


• • •
Missing some Tweet in this thread? You can try to
force a refresh