
1/ Interesting study comparing the metabolic effects of #fasting: lean vs. obese ppl
👉Lean have greater ⬆️ in Lipid Oxidation (+214% in lean vs. + 76% in obese at 48 hrs)
👉Resting energy expenditure ⬇️ in obese only
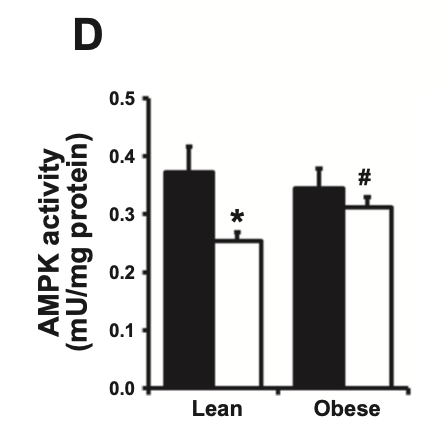
👉Skeletal muscle AMPK ⬇️ in lean
pubmed.ncbi.nlm.nih.gov/23512807/
👉Lean have greater ⬆️ in Lipid Oxidation (+214% in lean vs. + 76% in obese at 48 hrs)
👉Resting energy expenditure ⬇️ in obese only
👉Skeletal muscle AMPK ⬇️ in lean
pubmed.ncbi.nlm.nih.gov/23512807/

2/ Points 1 and 2 go in line with what I'd expect. Leaner metabolically healthy people probably have greater metabolic flexibility, resulting in better shift to fat burning. But point 3 about AMPK surprised me. Here's why...
3/AMPK is the cellular energy sensor. It's activated, in part by low energy status, i.e.
Decrease cellular energy supply increases AMPK activity
Seems paradoxical that in lean persons who r fasting AMPK activity goes DOWN, not UP, as if there is more energy when taking none in
Decrease cellular energy supply increases AMPK activity
Seems paradoxical that in lean persons who r fasting AMPK activity goes DOWN, not UP, as if there is more energy when taking none in
4/ "Surprisingly, AMPK-Thr172 phosphorylation, which was not different between groups at baseline, was reduced by fasting in lean but not in obese"

5/ Then in the discussion the speculate that this could be due to increased glycogen stores during a fast!!! Isn't that odd?!
I find that interesting because I actually find I have a lot of power after a fast, e.g. I could more easily do muscle ups clap push-ups etc. That's n=1
I find that interesting because I actually find I have a lot of power after a fast, e.g. I could more easily do muscle ups clap push-ups etc. That's n=1

6/ There is further interesting speculation as to mechanism/rationale & I encourage people to read this paper. Fun!
But one think I will point out is the they only looked at skeletal muscle AMPK. I'd bet you'd see VERY different things looking at fat cells and liver cells.
But one think I will point out is the they only looked at skeletal muscle AMPK. I'd bet you'd see VERY different things looking at fat cells and liver cells.

• • •
Missing some Tweet in this thread? You can try to
force a refresh




