Some thoughts from seeing a ton of Covid in the ER this week
Good news: Aside from a few patients with compromised immune systems, didn't have to hospitalize anyone who was vaxxed/boosted
Bad news: Health systems are stressed to the max
We need to adapt...quickly
Thread👇
Good news: Aside from a few patients with compromised immune systems, didn't have to hospitalize anyone who was vaxxed/boosted
Bad news: Health systems are stressed to the max
We need to adapt...quickly
Thread👇
Below I’m going to cover
1) Clinical presentations based on vax status
2) The 3 types of hospitalization: For Covid, chronic disease exacerbated by Covid, incidental Covid
3) Differences in severity/hospital needs
4) Disruptions in care Covid+ patients
5) Health system adaption
1) Clinical presentations based on vax status
2) The 3 types of hospitalization: For Covid, chronic disease exacerbated by Covid, incidental Covid
3) Differences in severity/hospital needs
4) Disruptions in care Covid+ patients
5) Health system adaption
This version of Covid is crazy contagious. Our ER hit record highs in patient volumes. Hospitals everywhere over capacity during this surge of people coming in with Covid.
There is a strikingly consistent pattern based on vax status…
There is a strikingly consistent pattern based on vax status…
Boosted? Hardly saw anyone who had gotten a booster because if they caught Covid they’re likely at home doing fine or having regular cold/flu like symptoms
Vaxxed/unboosted? Tons of patients like this: wiped out, dehydrated, febrile. If they were older (eg > 55 yo or had other medical problems) often had to admit for overnight IV hydration and supportive care. But usually go home within a day or two.
Unvaxxed: These are the folks that get sick and had to be hospitalized because they need oxygen, some even younger than me. Fortunately Philly has a fairly high vaccination rate, particularly in older adults, so we’re not seeing severe cases as much as we used to.
Covid is all around. Chances are you’ll get it at some point. I share these observations in case you’re on the fence about whether you want a booster or your first shot, or if you are fully boosted, that you have some peace of mind and feel less anxious. But...
...In the meantime, a jump in vaccination rates is not going fix this insane surge in cases we're seeing right now and for the next 4-6 weeks.
Health and social systems need to seriously adapt and quickly, or our ability to provide health care will be seriously compromised...
Health and social systems need to seriously adapt and quickly, or our ability to provide health care will be seriously compromised...
...First, this Covid wave is different and we need to be smarter about how we interpret Covid cases that present to the ER and subsequent hospitalizations numbers (which are through the roof). They fall into three categories and can be managed differently...
1) Hospitalized for Covid: mostly unvaxxed or elderly/chronic ill & unboosted
2) Covid exacerbated a chronic illness (e.g. COPD) aka "The Covid Tip” (h/t @jeremyfaust)
3) Incidental Covid (caught on screening) happens to everybody (maybe ~1/5 of hospitalizations I saw)...
2) Covid exacerbated a chronic illness (e.g. COPD) aka "The Covid Tip” (h/t @jeremyfaust)
3) Incidental Covid (caught on screening) happens to everybody (maybe ~1/5 of hospitalizations I saw)...
...Based on increased immunity in the population, and this lower severity strain of Covid, less people are presenting with a need for ICU level care.
But a HUGE number need supportive care over 1-3 days (e.g. IV fluids, brief oxygen support, optimization of chronic illness)...
But a HUGE number need supportive care over 1-3 days (e.g. IV fluids, brief oxygen support, optimization of chronic illness)...
...Second major difference in this wave is there a huge number of patients coming to the ER for testing with mild symptoms or even no symptoms because of the lack of available testing or timely outpatient evaluation capacity elsewhere...
...Lastly, the shear number of people testing positive with mild or no symptoms means there's a large population of patients with serious health needs that are having challenges accessing care because of their Covid + status...
...Dialysis patients report difficulty getting outpatient dialysis because they tested positive. Many psych crisis centers, detox units, homeless shelters, and some nursing facilities won’t accept Covid+ patients. This leads to extra time in the hospital to meet these needs...
...So what can health systems do over the next 4-6 weeks to deal with the surge?
1) Set up Covid testing and flu like illness clinics outside the ER to divert low severity patients from ERs to more convenient care and allow ERs to focus on non Covid and Covid emergency care...
1) Set up Covid testing and flu like illness clinics outside the ER to divert low severity patients from ERs to more convenient care and allow ERs to focus on non Covid and Covid emergency care...
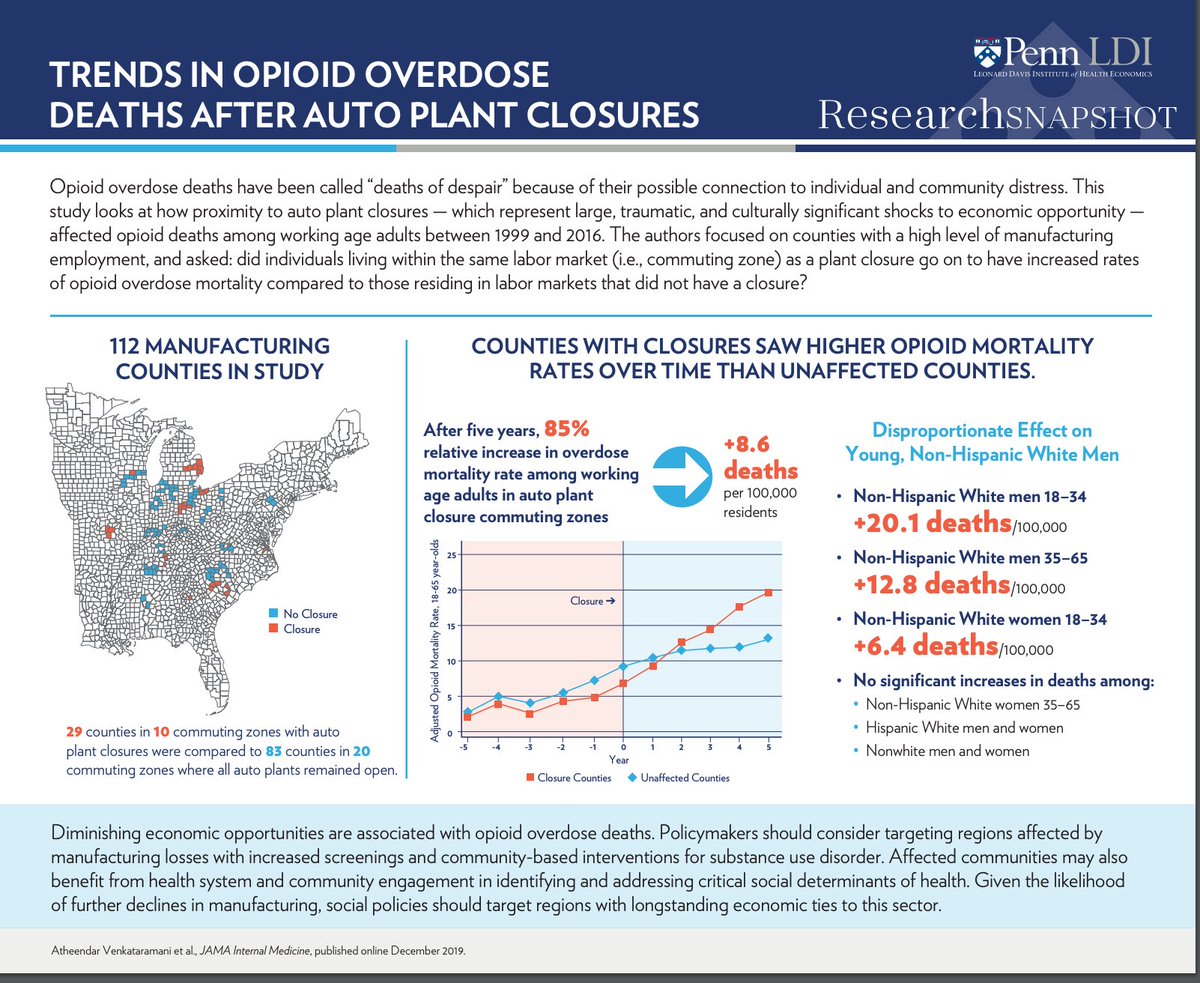
...2) Optimize care pathways in the hospital. We have shown the benefits of triaging lower severity patients (who are now the majority of hospitalizations) to dedicated Covid observation units. Better care, less time in the hospital. See article below...
https://twitter.com/kit_delgadoMD/status/1476415348375265280?s=20
...Another way to do this is to post a Hospitalist physician in the ER to help manage and optimize care for patients who are waiting for an inpatient bed to open up. By the time a bed opens up 24-48 hours later, the patient may be ready to be discharged from the ER...
...3) Dialysis centers, behavioral health treatment providers, and long term care providers need to adapt to the reality that a huge proportion of patients who need their care will incidentally test positive for Covid. Decreased access to care will worsen outcomes, and...
...and with staff in these facilities almost universally vaccinated and everyone wearing masks, the risks from Covid are no worse than any other aspect of society (family gatherings, public transportation, shopping, dining, bars, etc)...
...4) Finally, implementing a low-tech text-message based monitoring program can help the millions of patients who will test positive stay safe at home and get to the hospital at the right time if they get sick. See our work below...
pennmedicine.org/news/news-rele…
pennmedicine.org/news/news-rele…
......Thanks for reading. Hopefully by late Feb we will have more people boosted and access to new antivirals. Until then, things will be tough. Give us a hand in the hospital by helping to decrease the spread of Covid because right now it's unsustainable/
https://twitter.com/bhrenton/status/1477510685408047104?s=20
…PS - Fortunate to be part @Pennmedicine which has been very proactive in responding to this pandemic all along, increasing access vaccines, testing, remote monitoring and other innovations. But most of all, inspired by my colleagues. See thread below
https://twitter.com/kit_delgadoMD/status/1477436865632428036?s=20
..PS - Hospital and ER overcrowding, lack of bed capacity, and long ER waits are chronic problems made 100 times worse by Covid, omicron.
Here's the best piece explaining underlying causes and short and long term solutions:
Here's the best piece explaining underlying causes and short and long term solutions:
https://twitter.com/kit_delgadoMD/status/1443559587064463366
• • •
Missing some Tweet in this thread? You can try to
force a refresh