🧵Pleased to share our comprehensive review "#HFpEF: recent concepts in diagnosis, mechanisms & management", co-authored with @AndreasGevaert, incredible mentor @hvanspall, &⭐️collaborators @FaiezZANNAD @AndrewJSauer @HFpEF @kevin_damman @KSharmaMD
heart.bmj.com/content/early/…
heart.bmj.com/content/early/…
🧵First, we discuss the evolving definition of #HFpEF--> from LV hypertrophy with diastolic HF to arbitrary LVEF cut points of > 40% the > 50% to evolving concepts of HF phenotypes, beautifully illustrated in the figure below. @Heart_BMJ
heart.bmj.com/content/early/…
heart.bmj.com/content/early/…

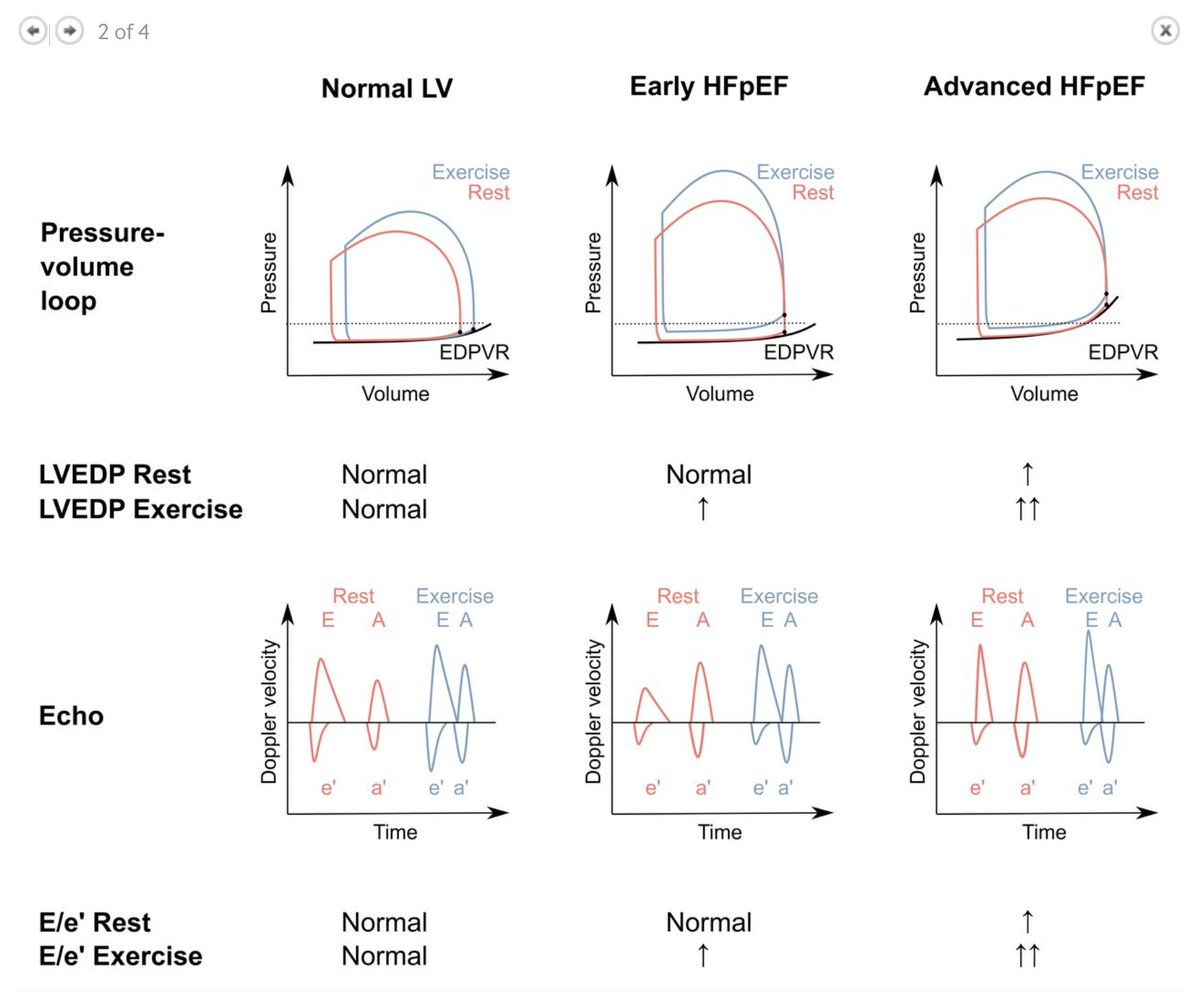
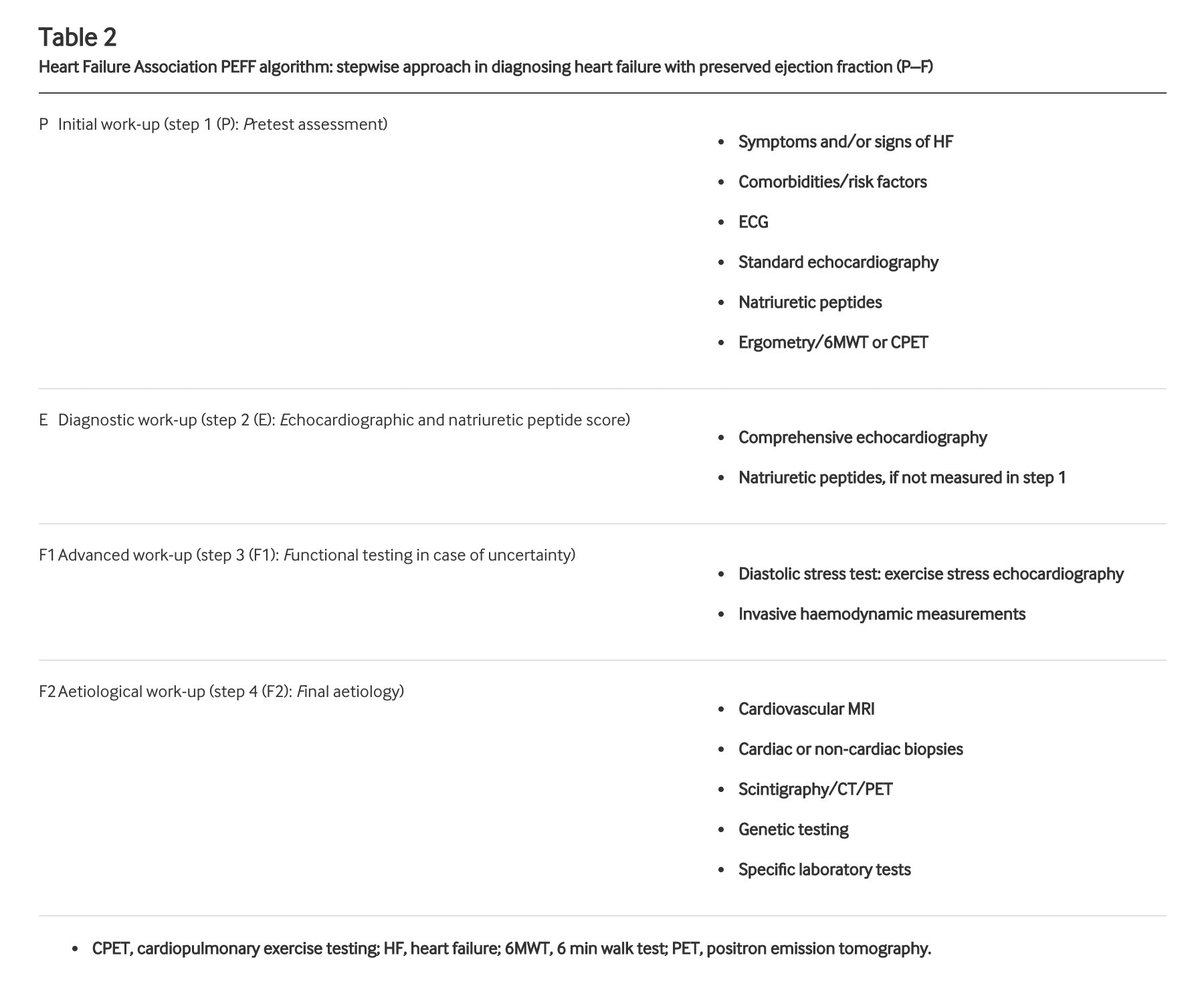
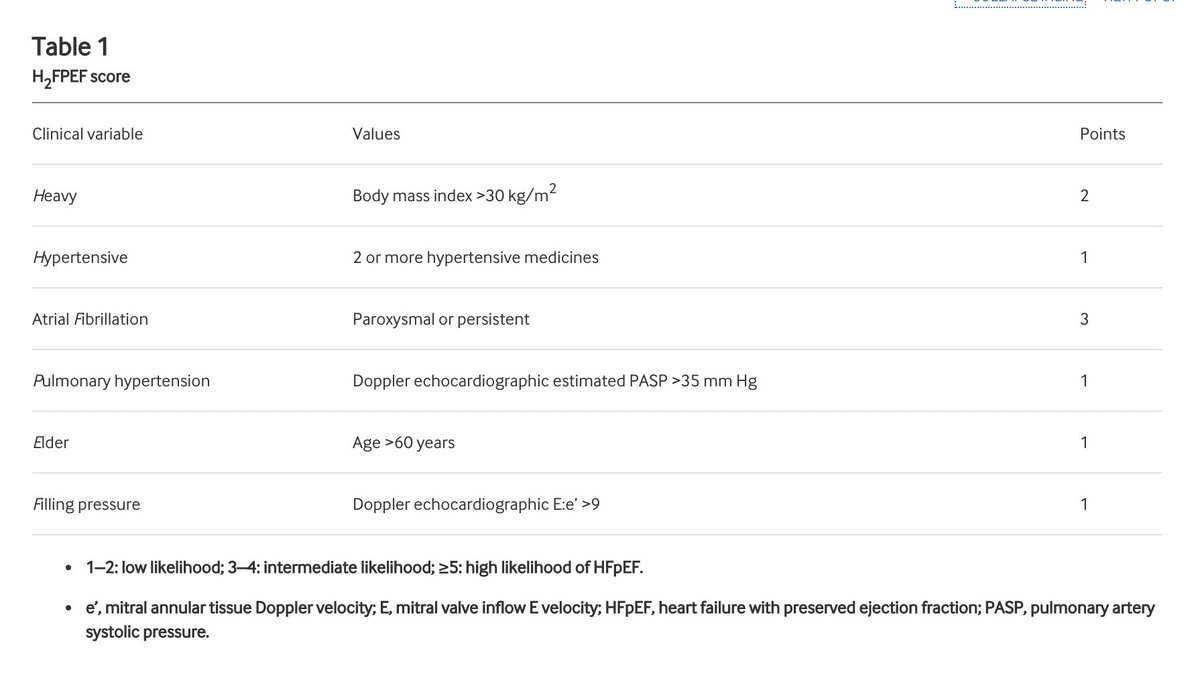
🧵We then review various approaches to making a diagnosis of #HFpEF--> symptoms and signs, utility of NT-proBNP, rest and exercise hemodynamics. We discuss existing diagnostic algorithms (H2FPEF and HFA-PEFF scores) and their applicability. @Heart_BMJ
heart.bmj.com/content/early/…
heart.bmj.com/content/early/…
🧵We present an extensive list of "#HFpEF mimickers" that MUST be ruled out before making a diagnosis of #HFpEF. @Heart_BMJ @MinnowWalsh @MiscSusan @HeartOTXHeartMD @ersied727 @AnastasiaSMihai @CardioIAN @WomenAs1 @Womenintxp_mcs @docbhardwaj @CVCTForum
heart.bmj.com/content/early/…
heart.bmj.com/content/early/…

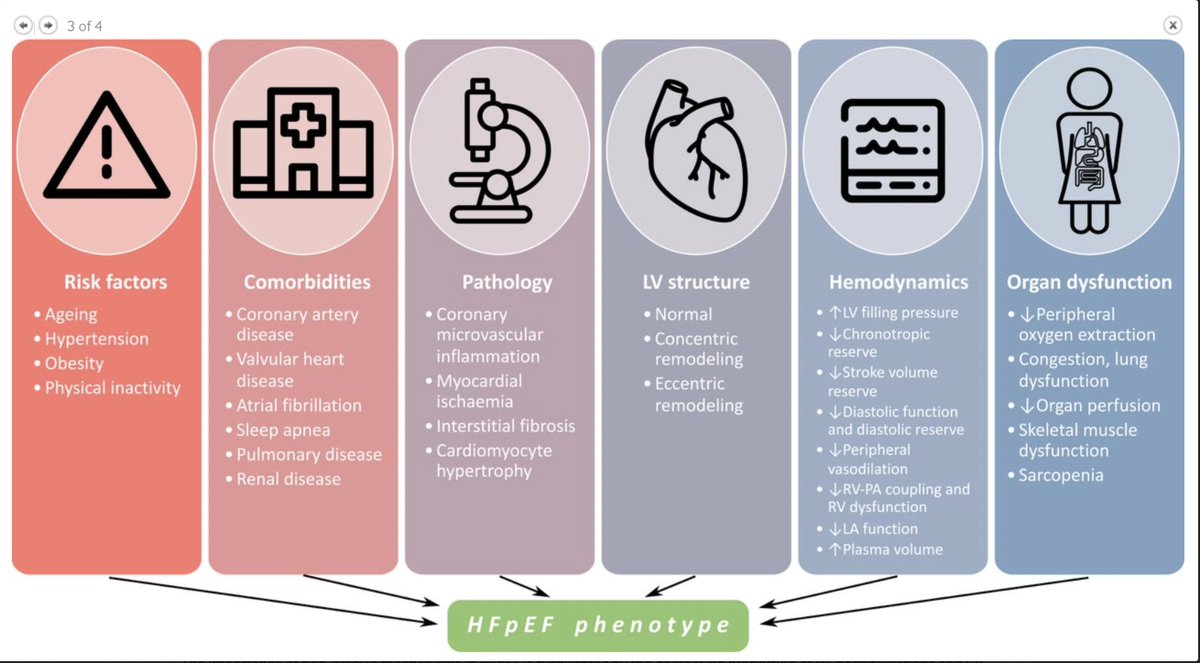
🧵We then describe recent insights in #HFpEF pathophysiology with a focus on the contribution and cardiac and non-cardiac mechanism and on #HFpEF phenotypes as illustrated below. @Heart_BMJ @ddefariayeh @GiselleSA_MDPhD @MGHHeartHealth @tonkhueMdPhd
heart.bmj.com/content/early/…
heart.bmj.com/content/early/…
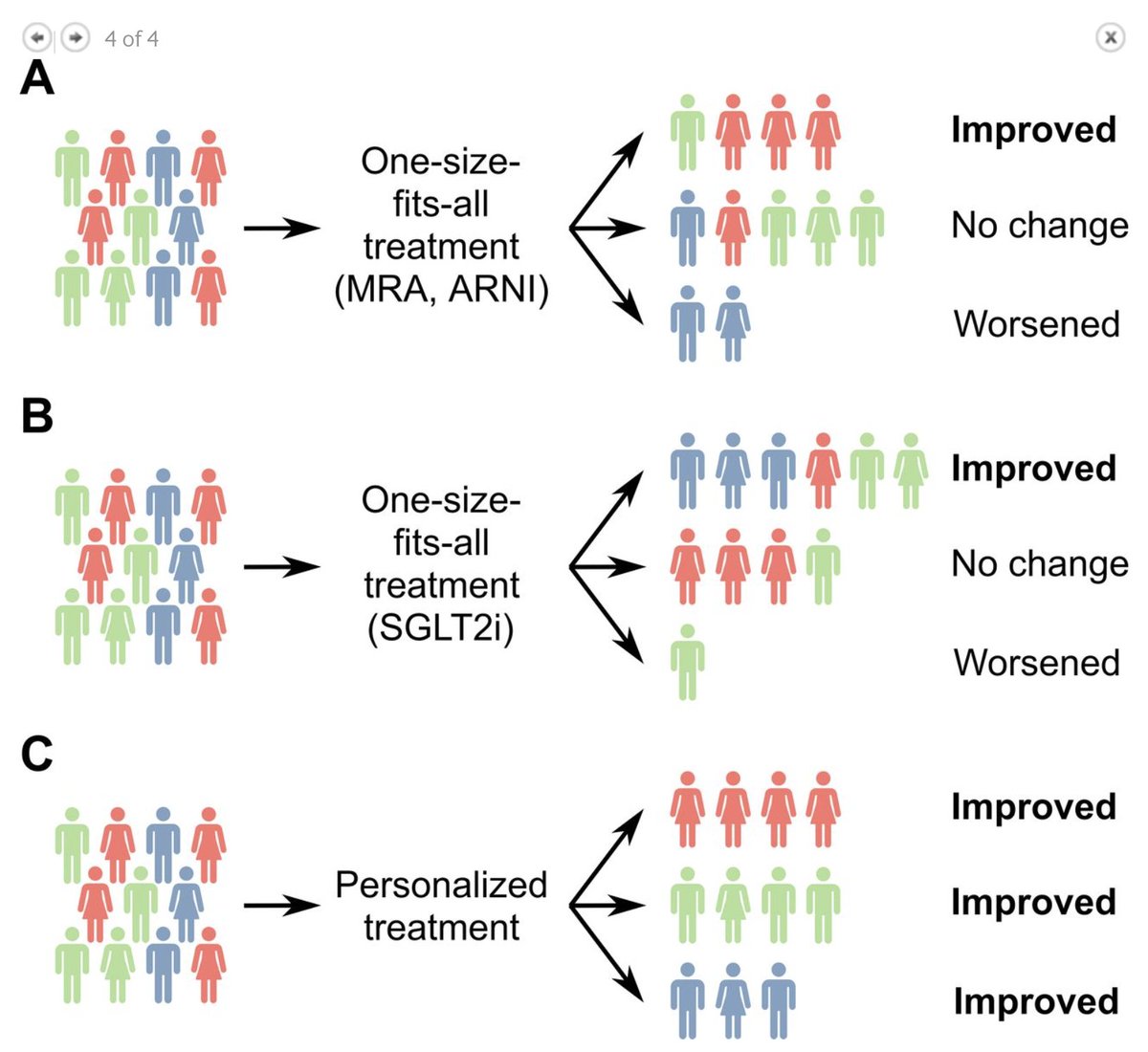
🧵Lastly, we discuss management of #HFpEF-lifestyle-based interventions, medical therapy, sex & race/ethnic differences, remote monitoring, & multidisciplinary care integration.
heart.bmj.com/content/early/…
I am deeply grateful to @hvanspall for being an incredible mentor & sponsor!
heart.bmj.com/content/early/…
I am deeply grateful to @hvanspall for being an incredible mentor & sponsor!
• • •
Missing some Tweet in this thread? You can try to
force a refresh