
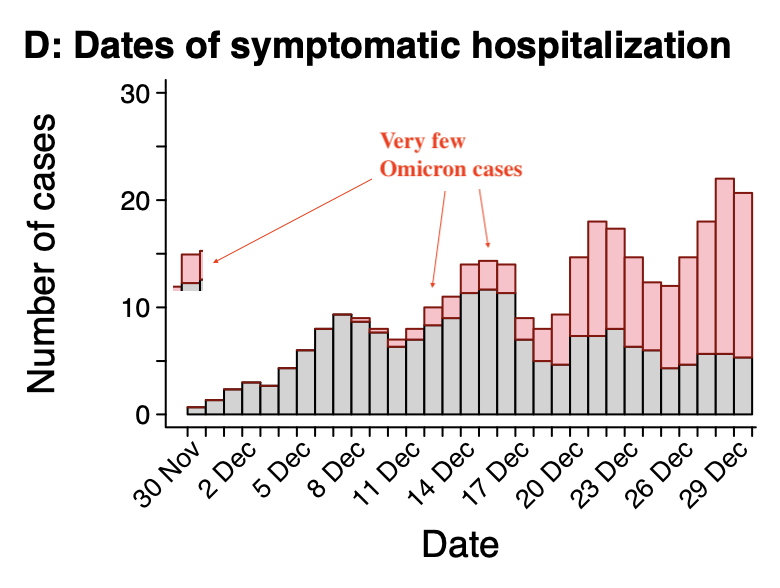
Context is missing and the information provided in this tweet is misleading: It takes time for people to progress to severe disease. Omicron cases in this study have an average observation period only of 5.5 days, compared to 15.8 days for Delta. 1/
https://twitter.com/CDCDirector/status/1481315911843856387
The study quoted treats this using a dynamic statistical (Cox) model but this doesn’t fix the limited data availability, whose analysis is limited to 14 days after infection. 2/
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
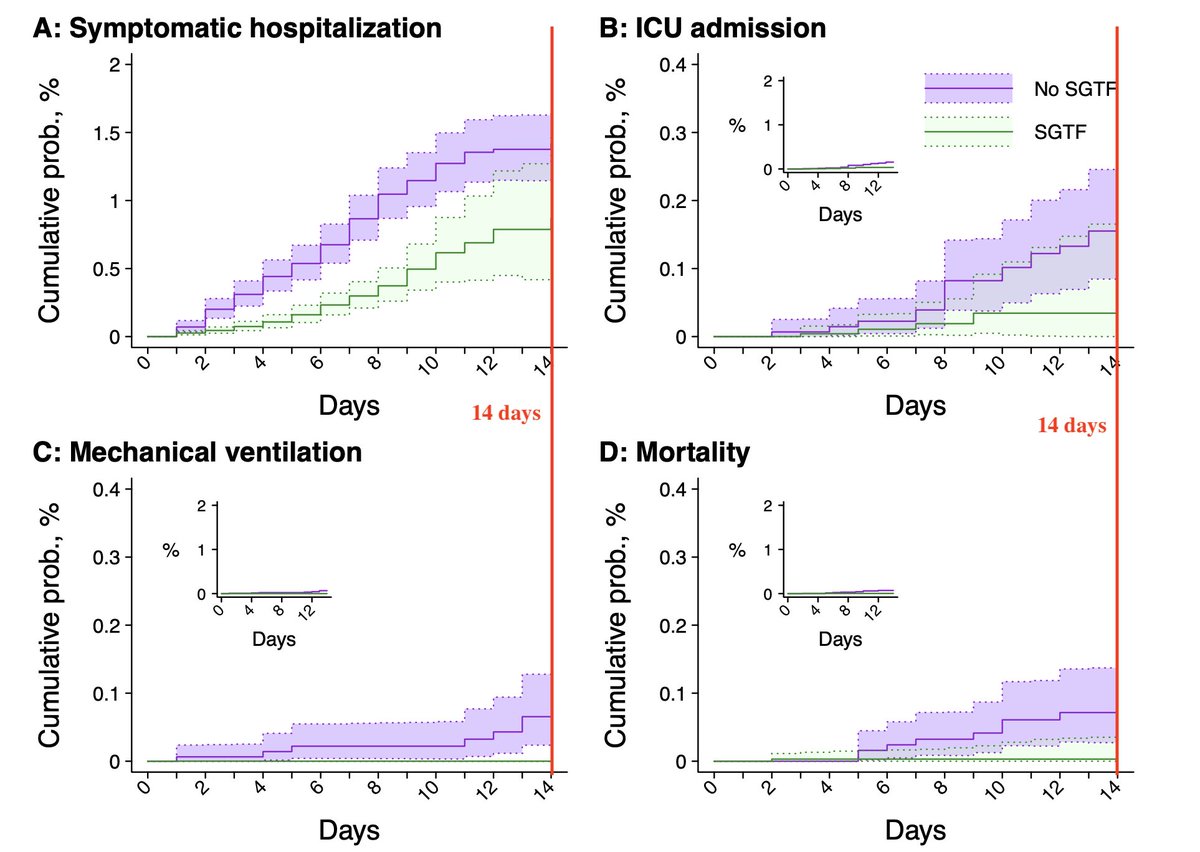
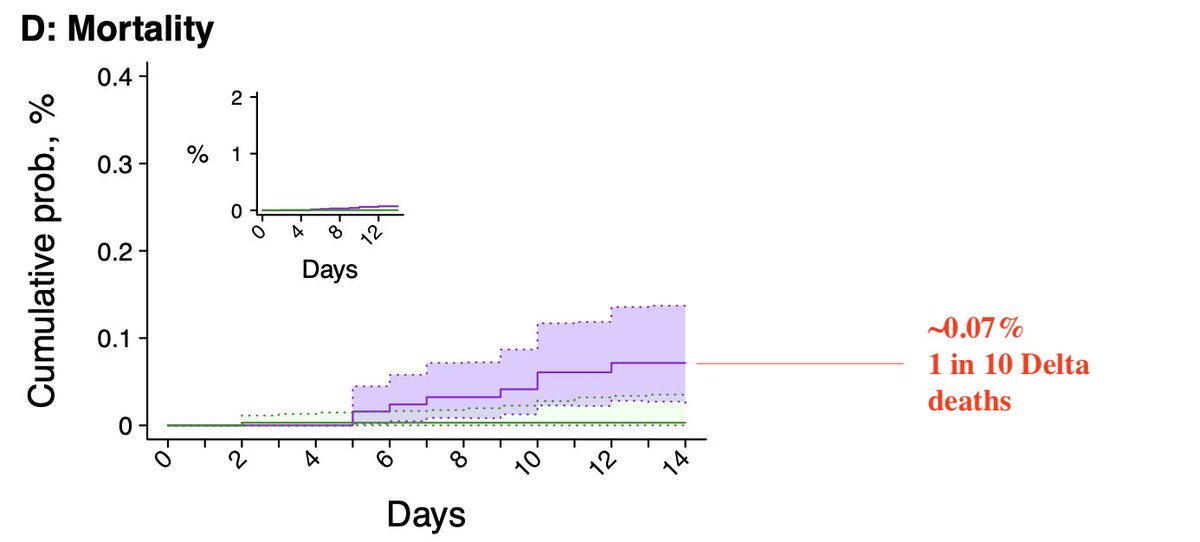
Essentially all Omicron hospitalizations start less than 14 days before study ends, limiting observation of severe cases & mortality, which generally take longer—less than 1 in 10 expected Delta deaths occur during these 14 days (14 day mortality ~0.07%, Nov US mortality .85%) 3/
This means uncertainty (error bars) for ICU & mortality are quite large—described in the study but not in the tweet—and the only statistical claim made by the study about mechanical ventilation is that it is less likely for Omicron than Delta 4/
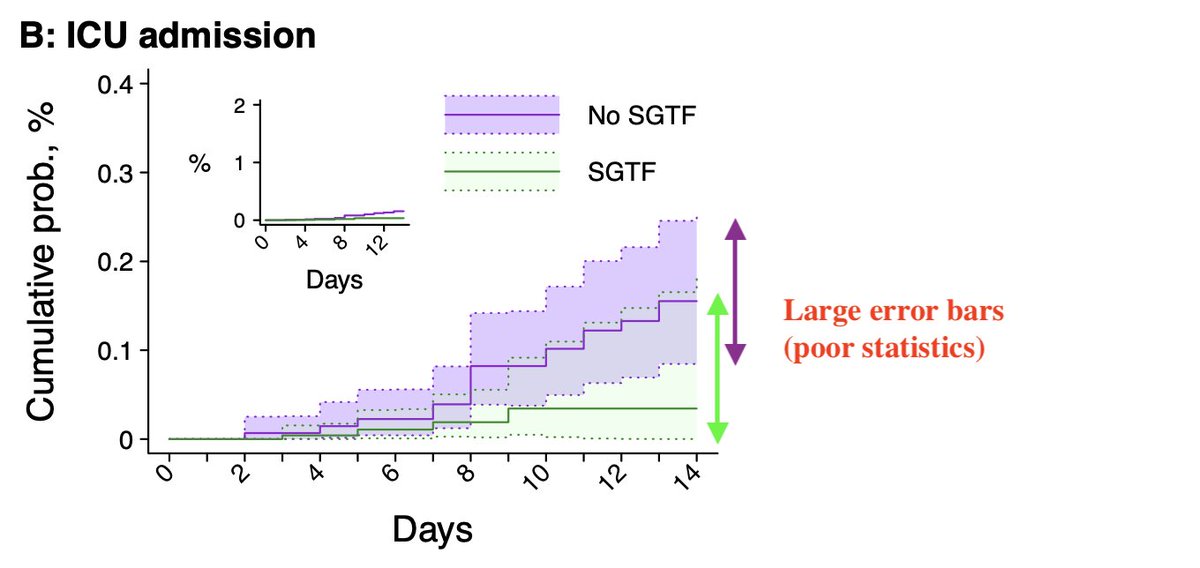
(i.e. the study acknowledges a lack of sufficient data to claim how much less likely). The initial tweet is very misleading. The information should be provided along with its statistical uncertainty, which is not provided. 5/
Also, study ICU, mortality & p-value for mechanical ventilation may be biased—significantly so—because, as reported in the study, omicron hospitalizations are younger & healthier compared to delta (perhaps due to these hospitalizations arising from initial set of omicron cases,6/
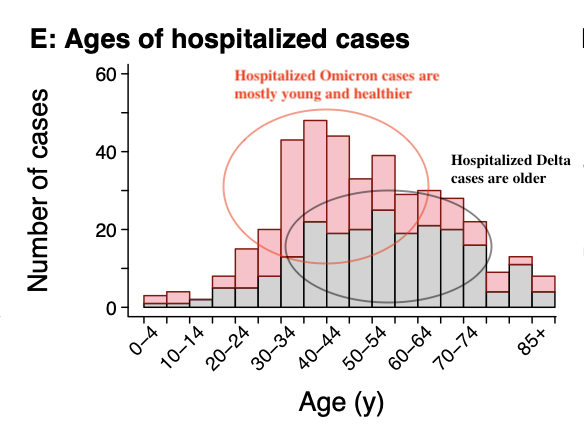
..which may differ in demographics from later cases), but ICU, mortality, & mechanical ventilation analyses, unlike hospitalization analysis, didn’t correct for demographic differences (the paper notes they didn’t have data to make multivariate corrections on these numbers). 7/
Current data from South Africa indicates continuing increase in mortality long after they would be expected to decline from the peak of cases. This suggests Omicron may have a longer delay to mortality than Delta, undermining the claims of this study. 8/
https://twitter.com/yaneerbaryam/status/1482518564682838019?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh







