
Results from our lab indicate that Omicron encodes a 2nd type of immune escape, besides the S mutations that evade antibody responses.
Background: Basically all cells of our body are able to produce interferons (IFNs) in response to infection. IFNs are secreted and dock...
1/11
Background: Basically all cells of our body are able to produce interferons (IFNs) in response to infection. IFNs are secreted and dock...
1/11
...onto their receptor on the neighbour cells. IFN activates a gene expression program that puts cells into an antiviral state. Instead of doing their normal job, they are now full of antiviral proteins to form a firewall and attract immune cells.
2/11
2/11
But: viruses have of course plenty of countermeasures in stock, mostly:
- suppressing IFN production in the infected cells
- disturbing the signaling between IFN receptor binding and the establishment of an antiviral state
- directly disarming antivirally active proteins
3/11
- suppressing IFN production in the infected cells
- disturbing the signaling between IFN receptor binding and the establishment of an antiviral state
- directly disarming antivirally active proteins
3/11
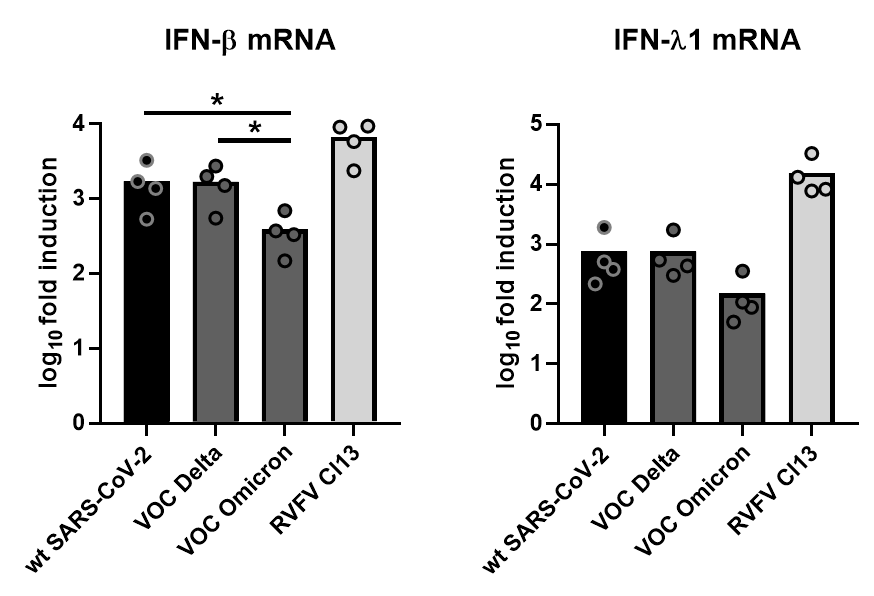
We checked IFN induction by cells that were infected with Omicron, in comparison to the original strain ("wt") and the Delta variant of concern
4/11
4/11
Result: one type of IFNs (IFN-beta), is about 4-fold less activated by Omicron. For the other type (IFN-lambda), there was no significant difference
5/11
5/11
How about the antiviral state? We also treated cells with different doses of IFN (dose escalation) before infection with the viruses.
Increasing doses of IFN are expected to generate more antiviral proteins, so it is increasingly harder for viruses to produce new particles
6/11
Increasing doses of IFN are expected to generate more antiviral proteins, so it is increasingly harder for viruses to produce new particles
6/11
Result:
For Omicron the IFN dose-response runs much flatter than for the other two viruses, indicating it is less impressed by the antiviral state established by IFN.
7/11
For Omicron the IFN dose-response runs much flatter than for the other two viruses, indicating it is less impressed by the antiviral state established by IFN.
7/11
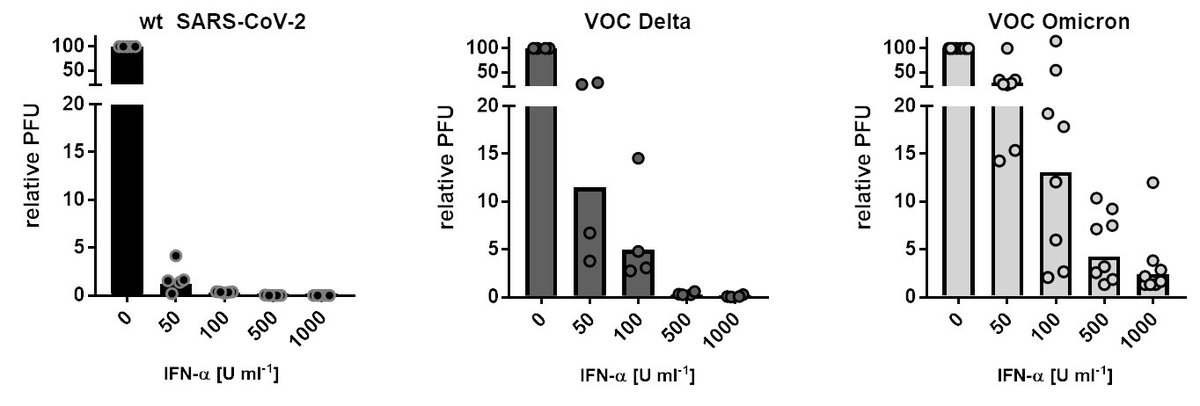
For example, for the wt SARS-CoV-2 you need just 50 units IFN to bring it below 5% of the normal virus amount. For Delta, you need about 100 units IFN to reach a similar suppression level, but for Omicron you have to use 500 units.
8/11
8/11
Together, our results indicate that Omicron has an increased capability to
- suppress IFN production
- evade the IFN antiviral state
As IFNs belong to the innate immune system, this is a kind of immune evasion
9/11
- suppress IFN production
- evade the IFN antiviral state
As IFNs belong to the innate immune system, this is a kind of immune evasion
9/11
BTW we have seen such a pattern earlier, when we found that wt SARS-CoV-2 from 2020 is more IFN sensitive than the "old" SARS-CoV-1 from 2003.
Apparently with the Omicron variant from end of 2021 SARS-CoV-2 has gained some ground meanwhile
10/11
jbc.org/article/S0021-…
Apparently with the Omicron variant from end of 2021 SARS-CoV-2 has gained some ground meanwhile
10/11
jbc.org/article/S0021-…
Great collaboration with @CiesekSandra and @marek_widera, incredibly hard and efficient work by my team members Lyudmila Shalamova and Ulrike Felgenhauer
11/11
biorxiv.org/content/10.110…
11/11
biorxiv.org/content/10.110…
• • •
Missing some Tweet in this thread? You can try to
force a refresh




