🇩🇰New important Danish data
-HIGHER rates of infection among vaccinated 5-11 yos, even when adjusting for testing rate
-Boosters not associated w/lower infection rates
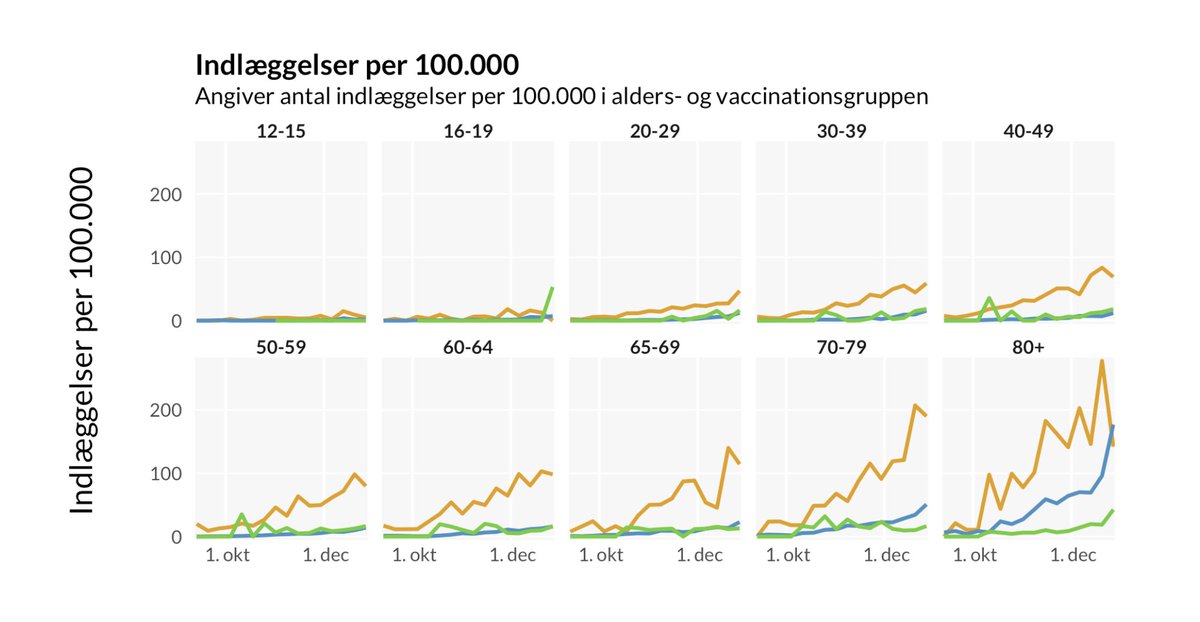
🟠unvaccinated
🔵2 doses
🟢booster
Data on severe disease & thoughts on mandates 👇
covid19danmark.dk/#gennembrudsin…
-HIGHER rates of infection among vaccinated 5-11 yos, even when adjusting for testing rate
-Boosters not associated w/lower infection rates
🟠unvaccinated
🔵2 doses
🟢booster
Data on severe disease & thoughts on mandates 👇
covid19danmark.dk/#gennembrudsin…

Here are COVID ICU (left) & hosp (right) admissions by vax category & age. Boosters have no clear association w/severe disease <age 40-50. This is consistent w/ Israeli data published in NEJM which found no significant correlation w/severe disease <age 40 nejm.org/doi/full/10.10…


Given the above, it's hard to argue college booster mandates are based in science. And, given even small risk of severe adverse events, are unethical. So this explanation 👇 sadly makes more sense than anything based in good public health or compassion
https://twitter.com/VPrasadMDMPH/status/1484706897160667139
& for kids 5-11 w/o comorbidities, simple precautionary principle: why should we chance any severe vax reactions for an incalculably low covid IFR & infection-hosp rate req treatment of <1/10,000 (less w/omicron) when vax doesn't prevent infection? medrxiv.org/content/10.110…

I think we are consistently seeing that vax/boosters don't prevent infection/give sterilizing immunity, but that number of vaccine doses should be targeted individually based on age and specific risk factors rather than mandated.
Data from @SSI_dk & @KT_Baek
Data from @SSI_dk & @KT_Baek
Many are asking about long covid and I will repeat what I have shared a number of times which is it has been found to be so rare in children that we can't even consistently detect it at the population level in well designed studies with control groups
https://twitter.com/TracyBethHoeg/status/1472670567228600320
Here are my thoughts on the most recent MISC data:
https://twitter.com/TracyBethHoeg/status/1485050166142930946
• • •
Missing some Tweet in this thread? You can try to
force a refresh