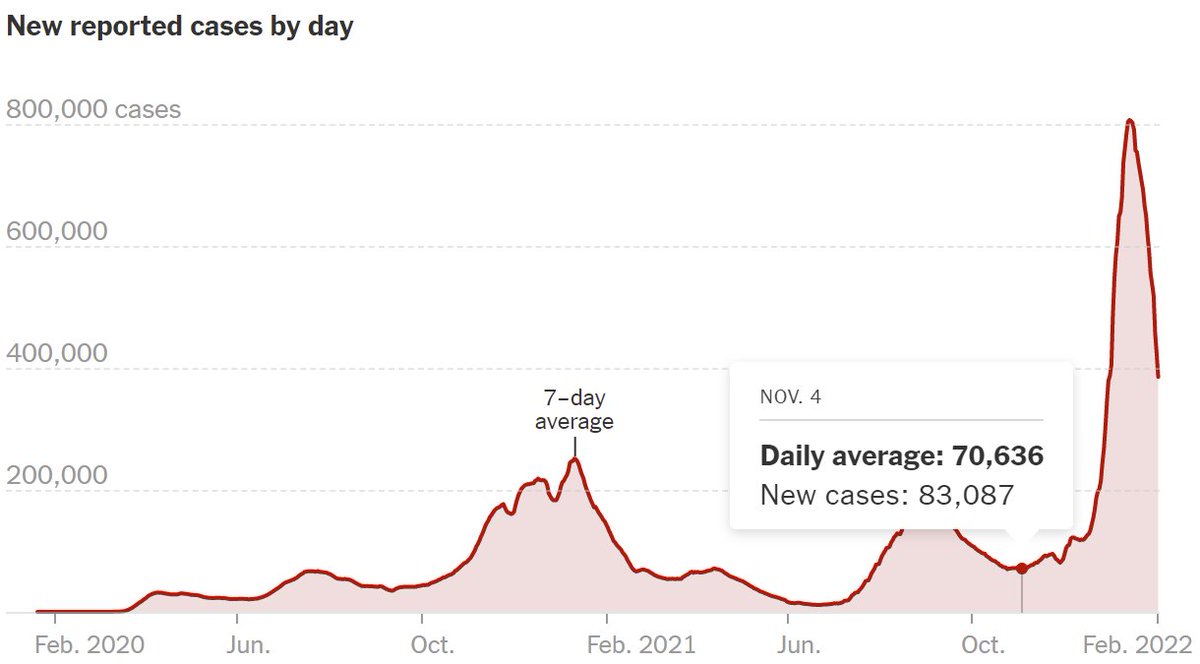
US COVID-19 deaths US >2000/day & continue to rise.
I can't help but wonder if focus on Omicron's mildness contributed to size of surge & deaths occurring now.
Difference in severity was small relative to higher infectiousness. Latter should have been singular focus of messaging.
I can't help but wonder if focus on Omicron's mildness contributed to size of surge & deaths occurring now.
Difference in severity was small relative to higher infectiousness. Latter should have been singular focus of messaging.

Obviously it would have been far worse if omicron had been as severe as Delta. But focus on mildness of Omicron by scientists, media, government, CDC, etc. contributed to people being less safe than they should have & now thousands are dying/day & many more w/ long covid
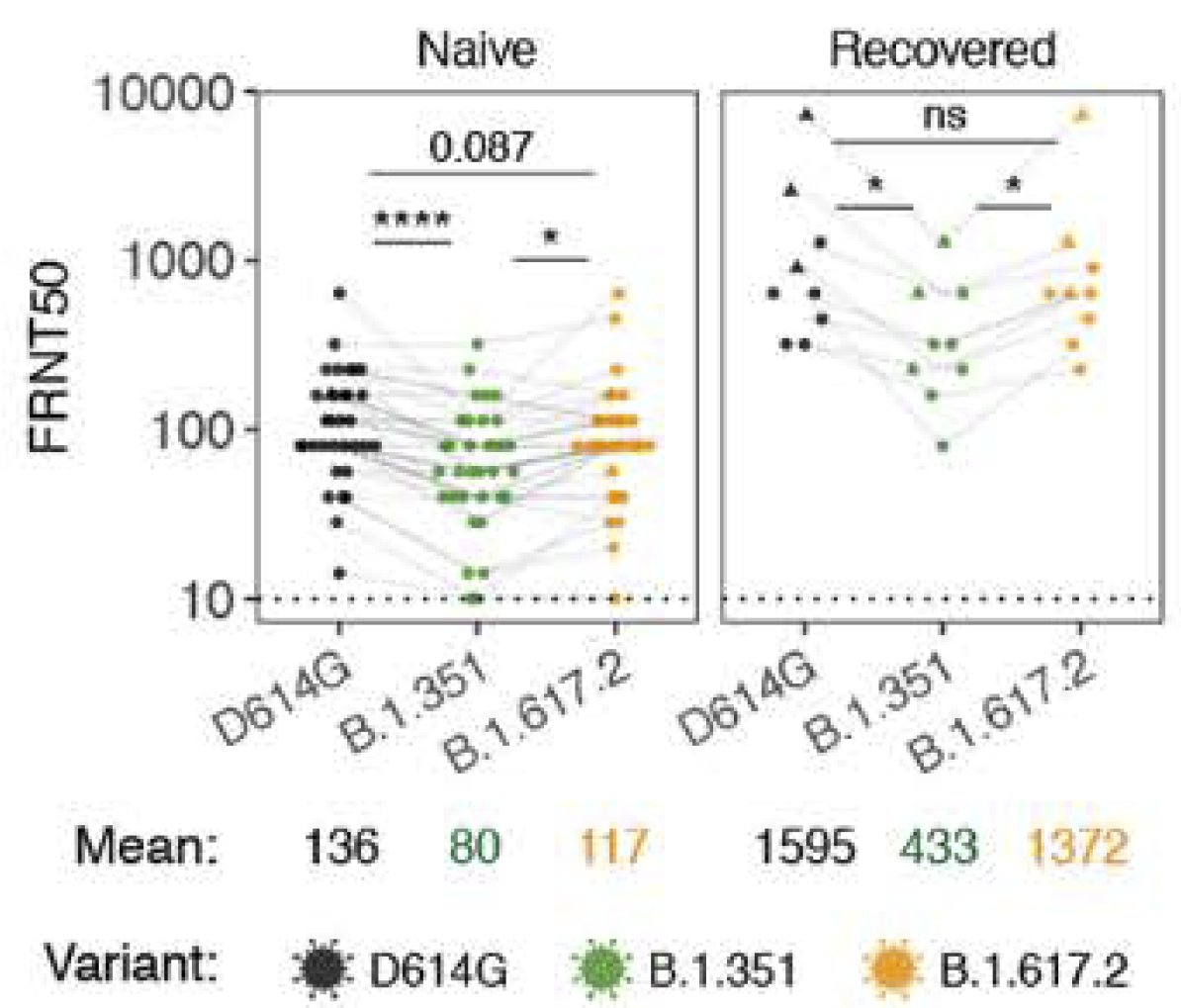
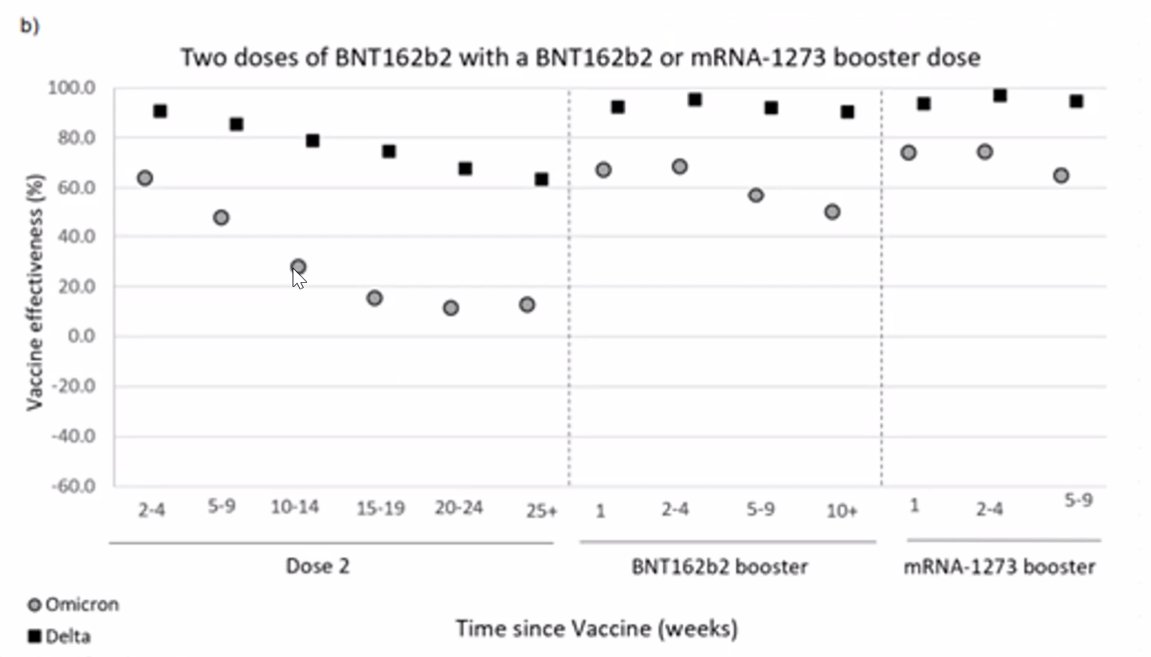
Biggest failure, in my opinion, was lackluster efforts to roll out 3rd dose boosters, which played huge role in much smaller impact of Omicron on deaths in UK & elsewhere.
In US, many scientists argued against need for boosters, possibly b/c of global vaccine equity issues.
In US, many scientists argued against need for boosters, possibly b/c of global vaccine equity issues.
However, science was clear that protection was waning & boosters were needed to reduce transmission. Boosters could have saved >10,000s of lives in Omicron surge. Denial of this science by many who knew better still bothers me deeply.
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
Vaccine inequity bothers me even more. I'm saddened progress has been so slow in getting vaccines to people who need them. Supply is no longer the issue. It's now about $$, despite cost to vaccinate world being tiny compared to impact. I contributed here:
gogiveone.org
gogiveone.org
Many people think Omicron surge is over (despite still having 400K cases/day in US!!!) & we can pretend pandemic is over, rather than redoubling our efforts to get people vaccinated & boosted. I wish there was more focus on a prospective approach.
For example, in Dec/Jan during Omicron surge US sent military doctors to help take care of patients. If US had sent military to vaccinate people in Oct/Nov, surge would have been smaller. Urgency to act is always too late.
• • •
Missing some Tweet in this thread? You can try to
force a refresh