How do we get broad immunity to SARS-CoV-2 that will protect against future variants?
2 studies (are there more?) suggest that vaccination followed by infection gives broader protection than infection followed by vaccination.
@florian_krammer @profshanecrotty @GuptaR_lab
2 studies (are there more?) suggest that vaccination followed by infection gives broader protection than infection followed by vaccination.
@florian_krammer @profshanecrotty @GuptaR_lab


1st paper (medrxiv.org/content/10.110…) shows: if you get vaccinated w/ mRNA vaccine & have a breakthrough Delta infection your subsequent antibodies are almost equally reactive in neutralizing Delta, Beta, Alpha, WT.

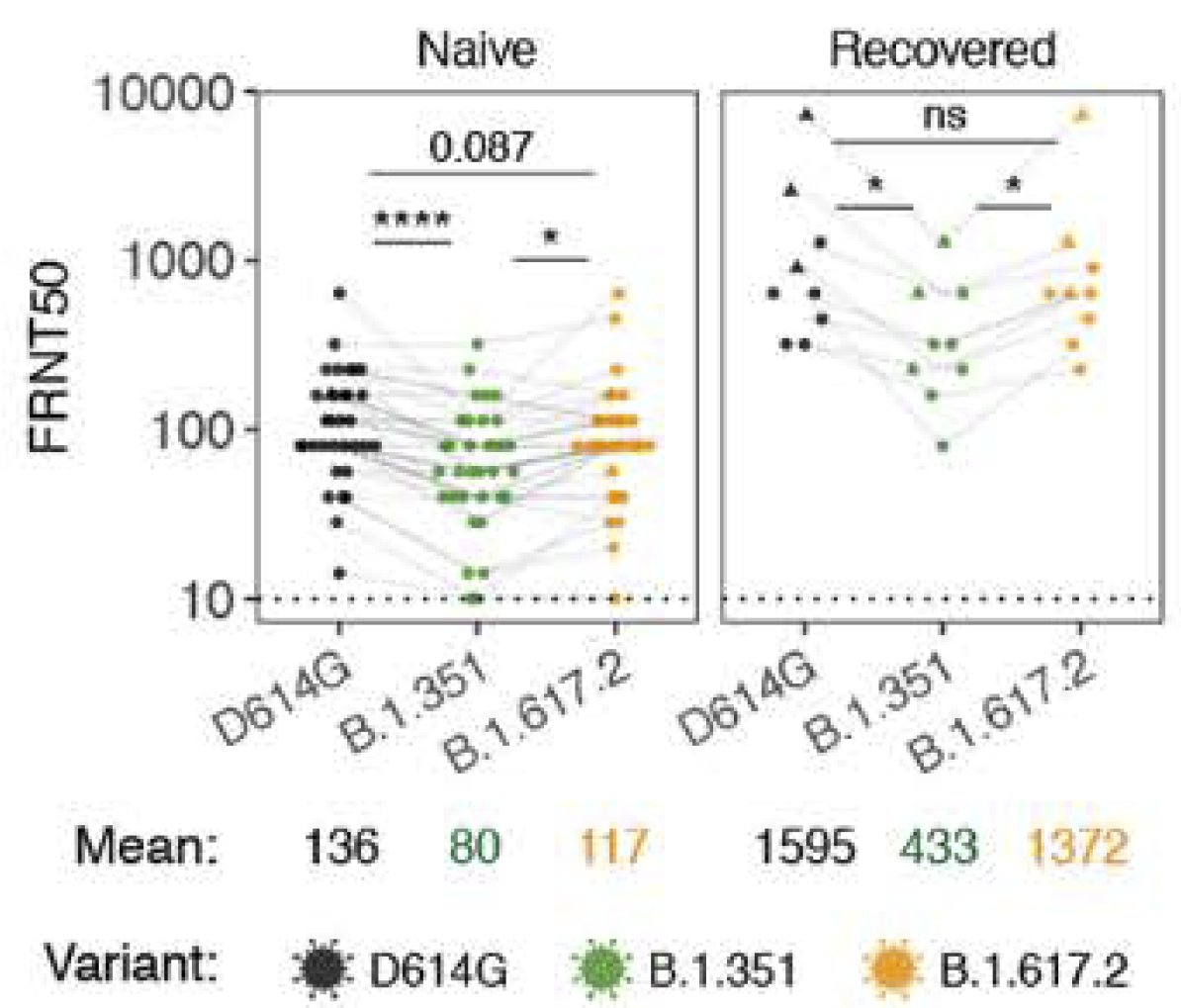
2nd paper (science.org/doi/10.1126/sc…) shows if you get infected (probably w/ D614G) then vaccinated w/ mRNA vaccine, your immunity is strong vs D614G & Delta but less so vs the most immune evasive variant so far, Beta.
It's unclear to me whether one could stimulate broad neutralizing antibodies seen in breakthrough cases using a vaccine with a different spike protein variant (e.g. Delta instead of Wuhan) or if broad response comes from exposure to the complete virus & can't be vaccine derived.
Caveat: Both studies have small sample sizes so difference might be due to chance & who knows if results vs Beta are indicative of whatever variant comes after Delta. But it's an important question & possibly 1 more reason its better to get vaccinated before getting exposed!
In case there was any confusion: it's much better to get your immunity to SARS-CoV-2 through vaccination rather than infection. That way you can avoid unpleasant side effects of infection like death and long covid.
• • •
Missing some Tweet in this thread? You can try to
force a refresh