Observations on new variant detected in Africa (Omicron)
-Many countries have closed borders, but I haven't heard of any that are simultaneously sending 10M vaccine doses to Africa.
-Closing borders while R>1 locally is silly. Virus is likely already widespread at v low freq.
-Many countries have closed borders, but I haven't heard of any that are simultaneously sending 10M vaccine doses to Africa.
-Closing borders while R>1 locally is silly. Virus is likely already widespread at v low freq.
-w/ no data, it's a bit shocking to see reputable people promoting 1 doctor's anecdotal observations that Omicron causes mild illness. If claim was opposite the same (always optimistic) scientist would demand to see data & suggest we don't believe it w/out rigorous analyses.
-interesting to see strong knee jerk reactions from reputable scientists (i.e. calling Omicron a scariant that we shouldn't worry about), while others take sequence data & mapping to make initial assessment that is worrisome:
https://twitter.com/florian_krammer/status/1464550752991514624
https://twitter.com/jbloom_lab/status/1464005676842184705
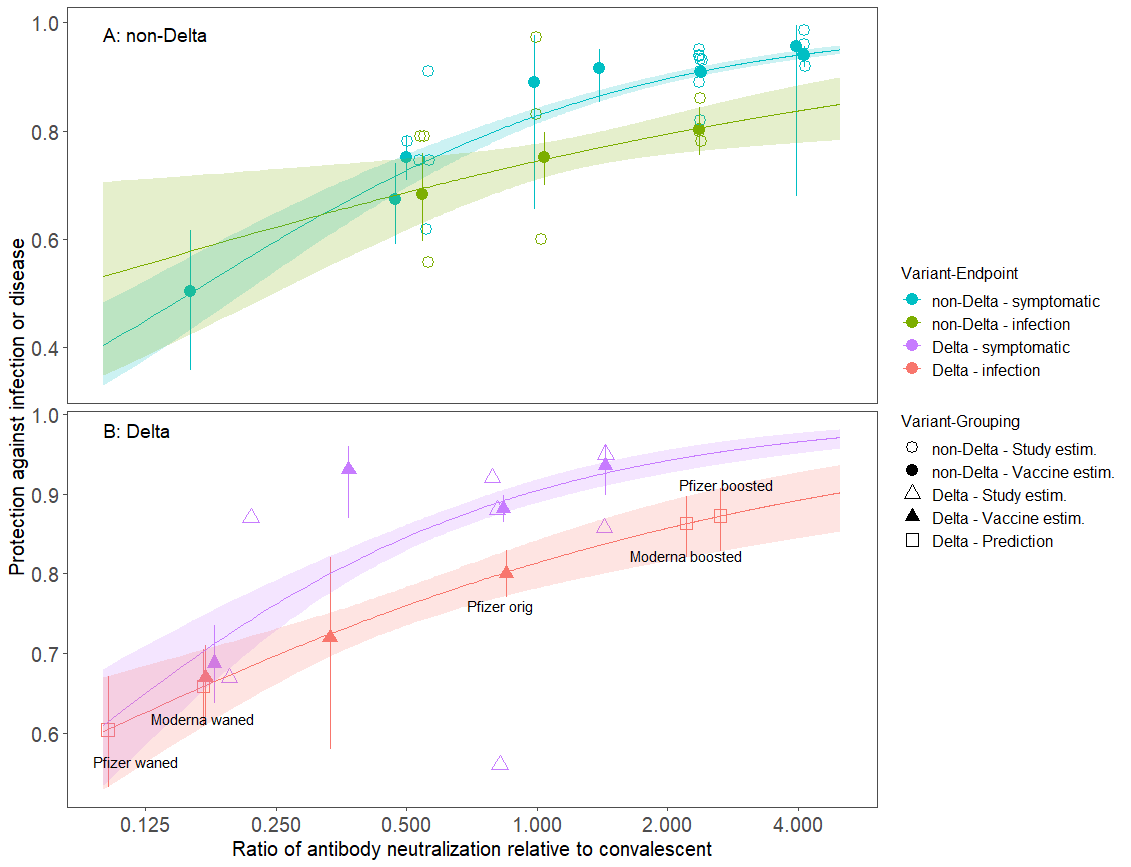
-lots of folks pre-judging studies underway of neutralizing antibodies as not very valuable, despite strong data linking neutralizing antibodies to efficacy of vaccines (doi.org/10.1038/s41591…; medrxiv.org/content/10.110…) 

-Some countries requiring 1 PCR test (sometimes post-arrival!) as if this will somehow stop introductions. It might reduce it a bit, but 1 test will miss many introductions. Only full 10d+ quarantine plus tests on day 10 will block most importations. @bencowling88
Here's what we know so far:
-Rise in cases in S Africa following subsiding of Delta wave (
-New variant detected (Omicron B.1.1.529) coincident w/ rise w/ many mutations of concern inc. mutations that increase infectiousness (
-Rise in cases in S Africa following subsiding of Delta wave (
https://twitter.com/Tuliodna/status/1463911554538160130).
-New variant detected (Omicron B.1.1.529) coincident w/ rise w/ many mutations of concern inc. mutations that increase infectiousness (
https://twitter.com/jbloom_lab/status/1464005676842184705)
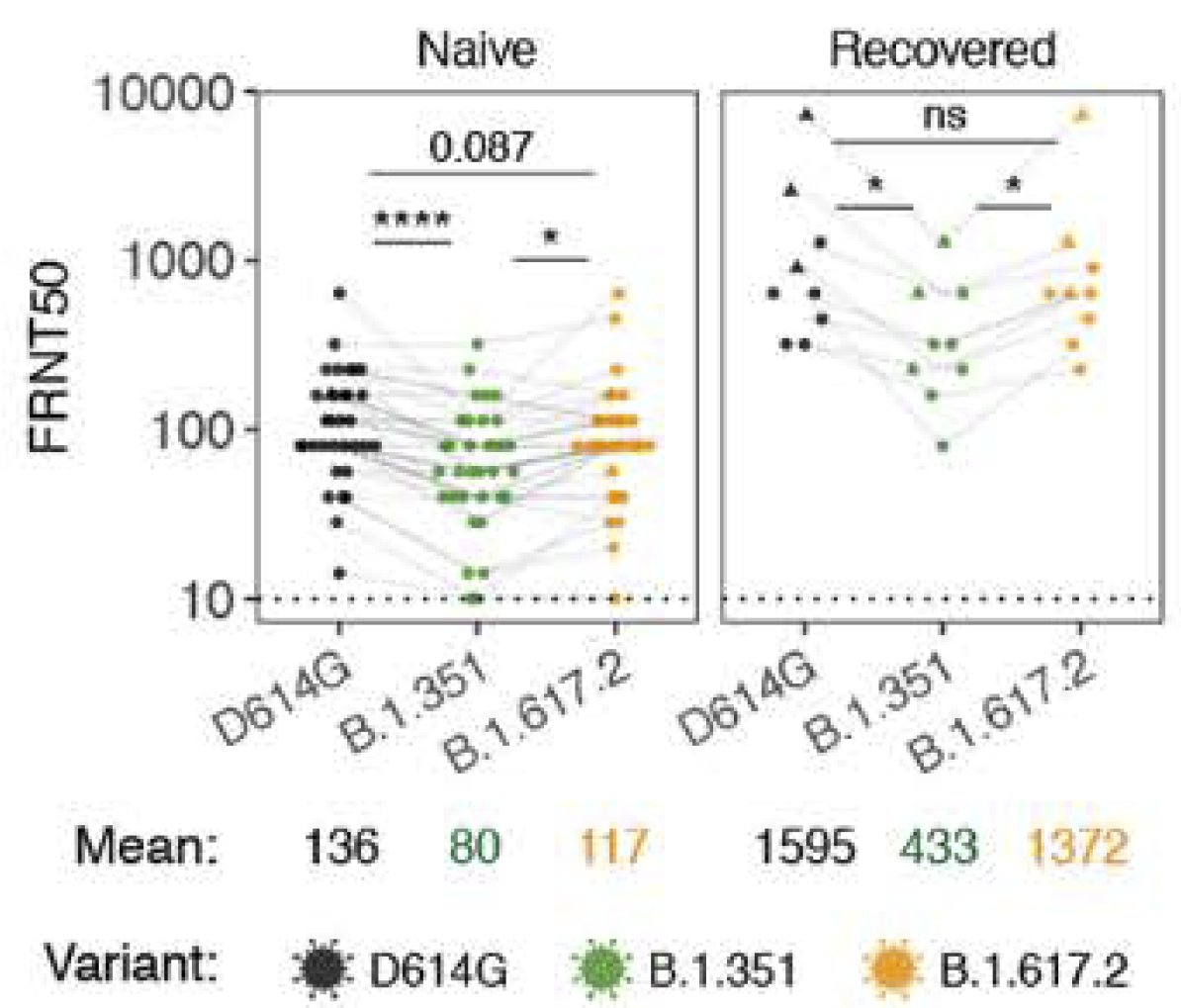
-Many Omicron mutations reduce antibody neutralization (
-Many Omicron mutations have unknown effects
https://twitter.com/theodora_nyc/status/1464257411582148608)
-Many Omicron mutations have unknown effects
What we don't know:
-Transmissibility of Omicron relative to Delta & contributions of infectiousness & immune escape (anyone seen data supporting higher prob of reinfection? who.int/news/item/26-1…)
-Differences in severity of illness
-Transmissibility of Omicron relative to Delta & contributions of infectiousness & immune escape (anyone seen data supporting higher prob of reinfection? who.int/news/item/26-1…)
-Differences in severity of illness
Since we don't have hard data on 3 things we want to know about new variants: transmissibility, immune escape, disease severity. What should we do?
-local precautionary approach: try to prevent establishment which requires reducing R/transmission via vaccines, masks, distancing &
-local precautionary approach: try to prevent establishment which requires reducing R/transmission via vaccines, masks, distancing &
reduce importation. Since variant is likely already widespread blocking travel from a few countries is ineffective. Need widespread quarantine & testing.
-global precautionary approach: immediately deploy vaccines in hardest hit areas (Africa)
-global precautionary approach: immediately deploy vaccines in hardest hit areas (Africa)
-medium term adaptation approach: develop vaccine booster specific to this variant; likely underway
-long term approach: deploy vaccines globally to reduce transmission & probability of future variants arising
-long term approach: deploy vaccines globally to reduce transmission & probability of future variants arising
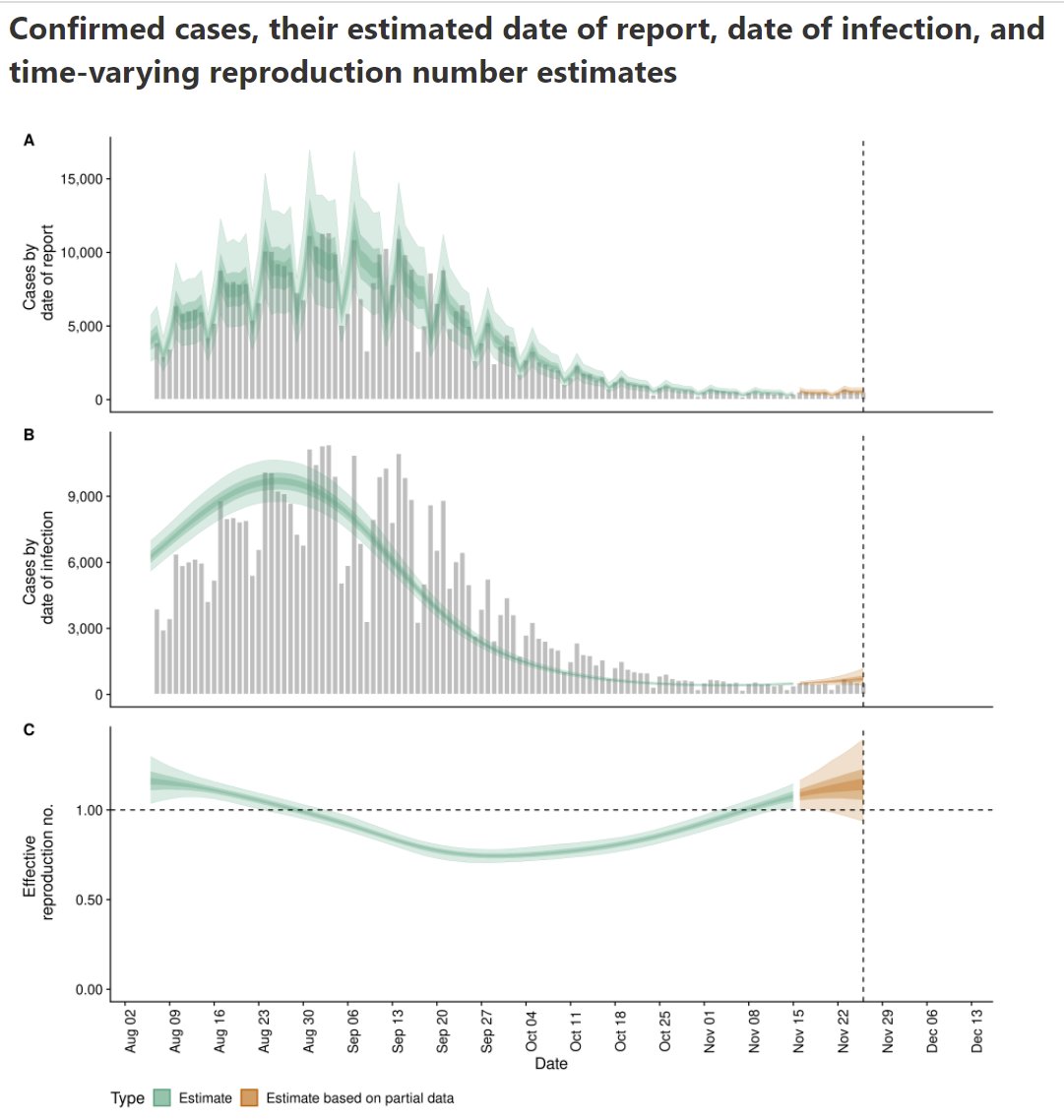
Example of ineffective approach discussed above (ban travel, when variant is already clearly locally established & Rt>1):
epiforecasts.io/covid/posts/na…
https://twitter.com/BNODesk/status/1464718106333491208
https://twitter.com/BNODesk/status/1464705335558651908
epiforecasts.io/covid/posts/na…
Evidence omicron is already widespread (please don't try to argue we are detecting and stopping all introductions)
https://twitter.com/Wikisteff/status/1464731580681887755?t=kZvoyx6jjM-52WK93Xntig&s=19
• • •
Missing some Tweet in this thread? You can try to
force a refresh