
How we treat smoldering multiple myeloma. @SagarLonialMD @mvmateos
@TheLancetHaem thelancet.com/journals/lanha… #myelomaVR
Summary of our recommendations below.
@TheLancetHaem thelancet.com/journals/lanha… #myelomaVR
Summary of our recommendations below.
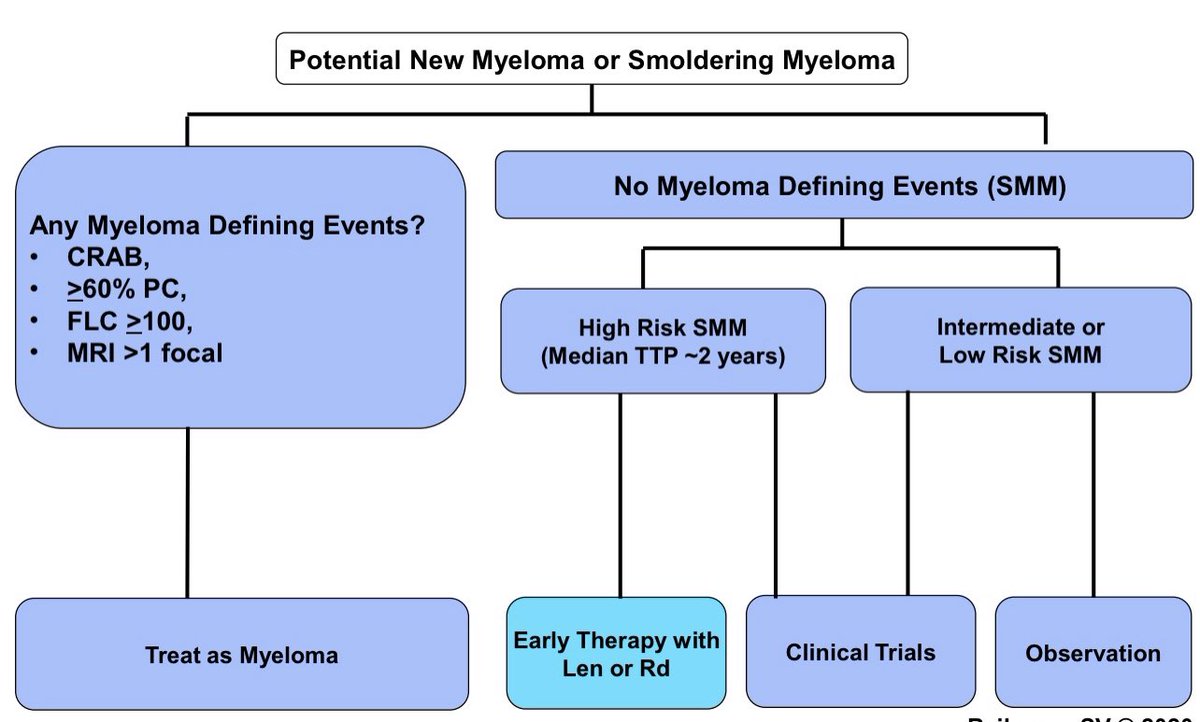
Risk stratification is based on the Mayo 20-2-20 system.
High risk is any 2 factors abnormal. These patients had 90% reduction in risk of end organ damage in the two RCTs of Len/Rd vs Observation. nature.com/articles/s4140…
High risk is any 2 factors abnormal. These patients had 90% reduction in risk of end organ damage in the two RCTs of Len/Rd vs Observation. nature.com/articles/s4140…

Approximately 1/3 of SMM is high risk.
If cytogenetics available use the IMWG scoring system. More precise estimate of risk. @mvmateos nature.com/articles/s4140… @BloodCancerJnl
If cytogenetics available use the IMWG scoring system. More precise estimate of risk. @mvmateos nature.com/articles/s4140… @BloodCancerJnl

Better than our algorithm is to enroll in a clinical trial. The current national RCT is comparing preventive approach with Rd to myeloma like treatment DRd. OS is the endpoint. @eaonc @nsc_natalie @mtmdphd
https://twitter.com/mtmdphd/status/1491423806271135748
Some people have asked me whether they can watch closely instead of treating high risk SMM. That's what we thought. We watched patients monthly. But we failed to prevent end organ damage: >90% reduction in end organ damage with Len compared to observation in our RCTs.
Unless you plan to see your patients every day you won't be able to prevent end organ damage in high risk smoldering myeloma in time.
And some if it will not be reversible.
And some if it will not be reversible.
When I have reviewed 1000s of medical records of smoldering myeloma patients being watched I always saw the confidence of the treating physician that all is well. Until it was not.
I don't make recommendations lightly without taking into account all possible pros and cons and factors. And I feel strongly that newly diagnosed patients with high risk smoldering myeloma should be offered early therapy.
The three of us, and our colleagues @myelomaMD @nsc_natalie and others are leading multiple trials including RCTs in smoldering myeloma. It's not easy to run these trials. It's not easy to design and get these approved and accrued.
We will continue to report our findings.
We will continue to report our findings.
2 years and stop. That what we recommend in the paper. And that's what we are doing in the ongoing ECOG phase III.
Adding my response to a question I had at ASH:
If you say "Ill watch the patient carefully, and Ill catch progression before it happens," that experiment was done and it failed. In 2 RCTs. In the US and Spain.
Patients should not be placed at risk of end organ damage.
If you say "Ill watch the patient carefully, and Ill catch progression before it happens," that experiment was done and it failed. In 2 RCTs. In the US and Spain.
Patients should not be placed at risk of end organ damage.
• • •
Missing some Tweet in this thread? You can try to
force a refresh











