
🧵on easing #Covid19 restrictions when Omicron appears to be exiting in many parts of Canada but the pandemic has not. Time to pool our efforts & invest honestly towards sustainable safety, minimal disruption/collateral damage. 1/
Ontario Sci Table data showing lots of positive trends right now. Wastewater signal, hospitalizations, ICU admission, deaths, all on the decline. But a trend is just that. Right direction. Not the finish line. Trends change & 5 waves are proof of that. 2/ 


Several reasons for caution before assuming the worst is behind us:
Unfinished winter + lifting indoor gathering limits + incomplete vaccine coverage = guaranteed spikes in transmission. Only ?s are how much & how soon. 3/
Unfinished winter + lifting indoor gathering limits + incomplete vaccine coverage = guaranteed spikes in transmission. Only ?s are how much & how soon. 3/
W/ testing limited, case counts are of almost no value. The canary in the mine is reduced to wastewater signal (where available). PH measures can't be enacted only when lagging indicators hospitalization/ICU/deaths arrive. Every wave burned us like this. 4/
Omicron will keep targeting those not optimally protected (< 3 doses). 3-dose coverage in Ontario: 45% overall. 2-dose coverage age 5-11: 22%. < age 5 vaccination won't start for a few weeks minimum. (NB "Full" 👇means TWO not 3 doses) 5/

IMPORTANT: Immunity via prior infection or prior variants doesn't reliably offer the same to the successor variant. Omicron demonstrates this clearly - can we confidently say the next variant won't up the ante further? 6/

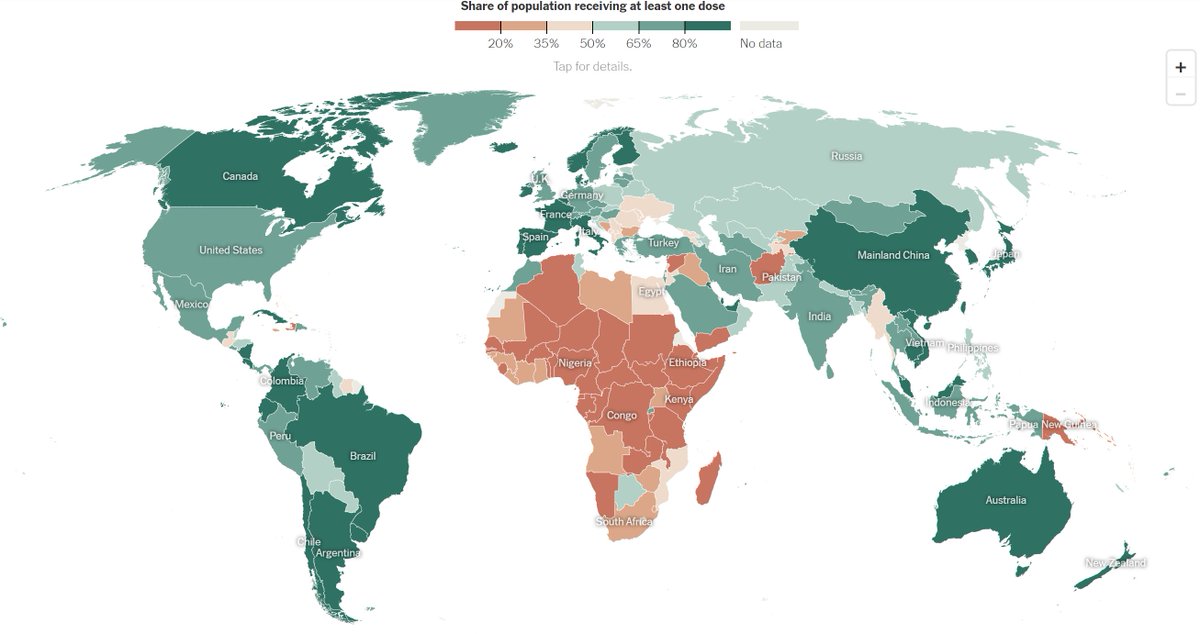
ENDemic is such a tempting descriptive, right? Problem is that PANdemic means it's still devastating much of the planet that is under-resourced. Future variants & waves everywhere will continue if this continues without meaningful #VaccineEquity 7/
Do we want a perpetual cycle of tribalism, polarizing narratives, pitting ourselves against each other in a (supposed) zero sum game of freedom/mental health/kids/schools/science/healthcare/globalism? No. An inch of common ground beats a mile of hate. 8/
Be smart. Easing restrictions means you "can" but doesn't mean you "should". Legal doesn't mean ideal or even safe in every context. Masking w/ N95-grade, ventilation awareness & vaccine uptake opportunity still matter. Thread's over. #COVID19 isn't. End/9
• • •
Missing some Tweet in this thread? You can try to
force a refresh



