Delighted to share visiting scholar's @Timothee_MD latest paper
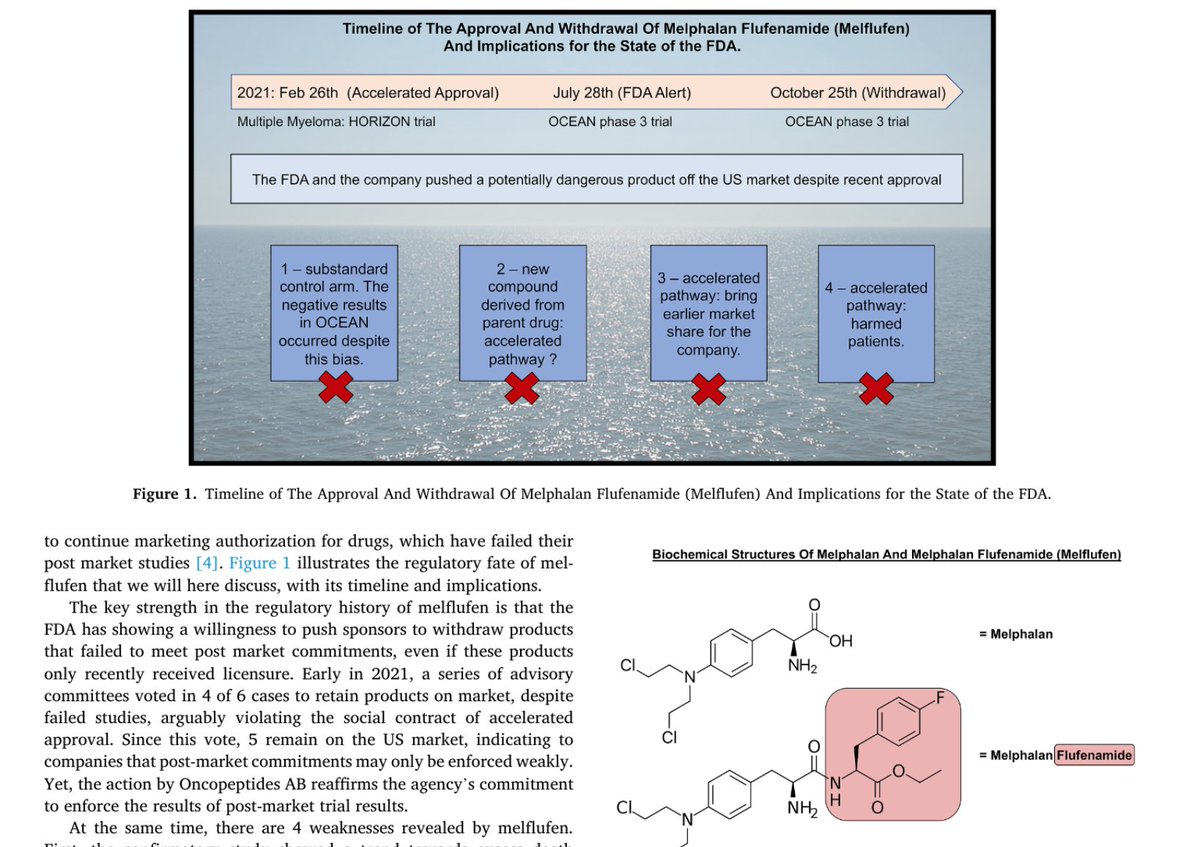
We analyze a FDA failure: The rapid approval of "totally novel" Melflufen based on surrogate 👇
Followed by withdrawal b/c of increased deaths <8 mo later!
What is going on at FDA?
authors.elsevier.com/sd/article/S19…
We analyze a FDA failure: The rapid approval of "totally novel" Melflufen based on surrogate 👇
Followed by withdrawal b/c of increased deaths <8 mo later!
What is going on at FDA?
authors.elsevier.com/sd/article/S19…
First, of all there are many many treatment options, many many ongoing trials, and countless combinations already available to treat myeloma
Yes, we need new drugs, but we can wait for RCTs to show they extend survival, we don't need to use broken surrogates like response
Yes, we need new drugs, but we can wait for RCTs to show they extend survival, we don't need to use broken surrogates like response
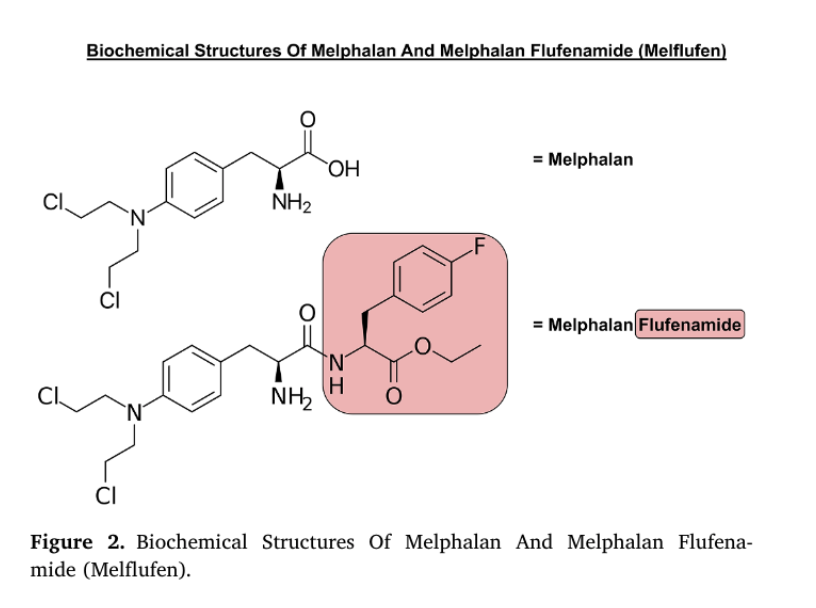
Second, melflufen is like me-too melphalan, a drug used for decades.
The drug was approved based on uncontrolled response rate of 23.5%, but what if you just gave pts a different, older alkylator?
The drug was approved based on uncontrolled response rate of 23.5%, but what if you just gave pts a different, older alkylator?
FDA threw the company a bone and let them run the OCEANS confirmatory trial without pre-treatment with dara (already proven drug), and against a doublet, which is beneath standard of care
It was a lay up
It was a lay up
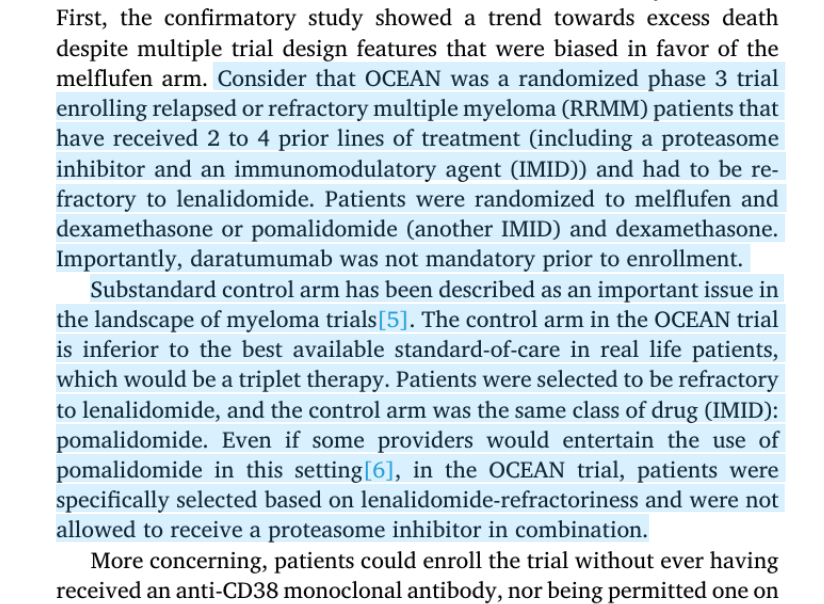
But despite this Ocean was halted b/c the experimental drug INCREASED death. Against a control arm BENEATH the US standard.
Wowzers!
Wowzers!

All this happened within 8 months!
What are we doing in drug regulation;
Why accept a surrogate when hard endpoints are coming?
And actually..
What are we doing in drug regulation;
Why accept a surrogate when hard endpoints are coming?
And actually..

Previously Chen & I proved that in these latter lines
that surrogates don't save time
Learn why here:
jamanetwork.com/journals/jamai…
that surrogates don't save time
Learn why here:
jamanetwork.com/journals/jamai…
Bottom line: Crediting the FDA for rapid withdrawal is a mistake, b/c they didn't need to grant approval in the first place
It is like crediting them for waiting for Kids vax <5, when they got you excited for no good reason in the first place
It is like crediting them for waiting for Kids vax <5, when they got you excited for no good reason in the first place
FDA is arsonist and firefighter in the Melflufen case
Drug regulation serves corporate interests & not cancer patients
This applies to other decisions as well
Sadly too few see the truth
Read the essay or Malignant book & follow @vkprasadlab
authors.elsevier.com/sd/article/S19…
Drug regulation serves corporate interests & not cancer patients
This applies to other decisions as well
Sadly too few see the truth
Read the essay or Malignant book & follow @vkprasadlab
authors.elsevier.com/sd/article/S19…
• • •
Missing some Tweet in this thread? You can try to
force a refresh