Summary tweet on my approach to anemias. credit to @n_gangat, @RichGodby, @zhuoerxie, Dr Ron Go, @VincentRK for teaching. Comments/critiques welcome!
1. Approach to anemia
1. Approach to anemia

2. Approach to iron deficiency anemia


4. Tests for hemolytic anemia

5. Differentials for autoimmune hemolytic anemia

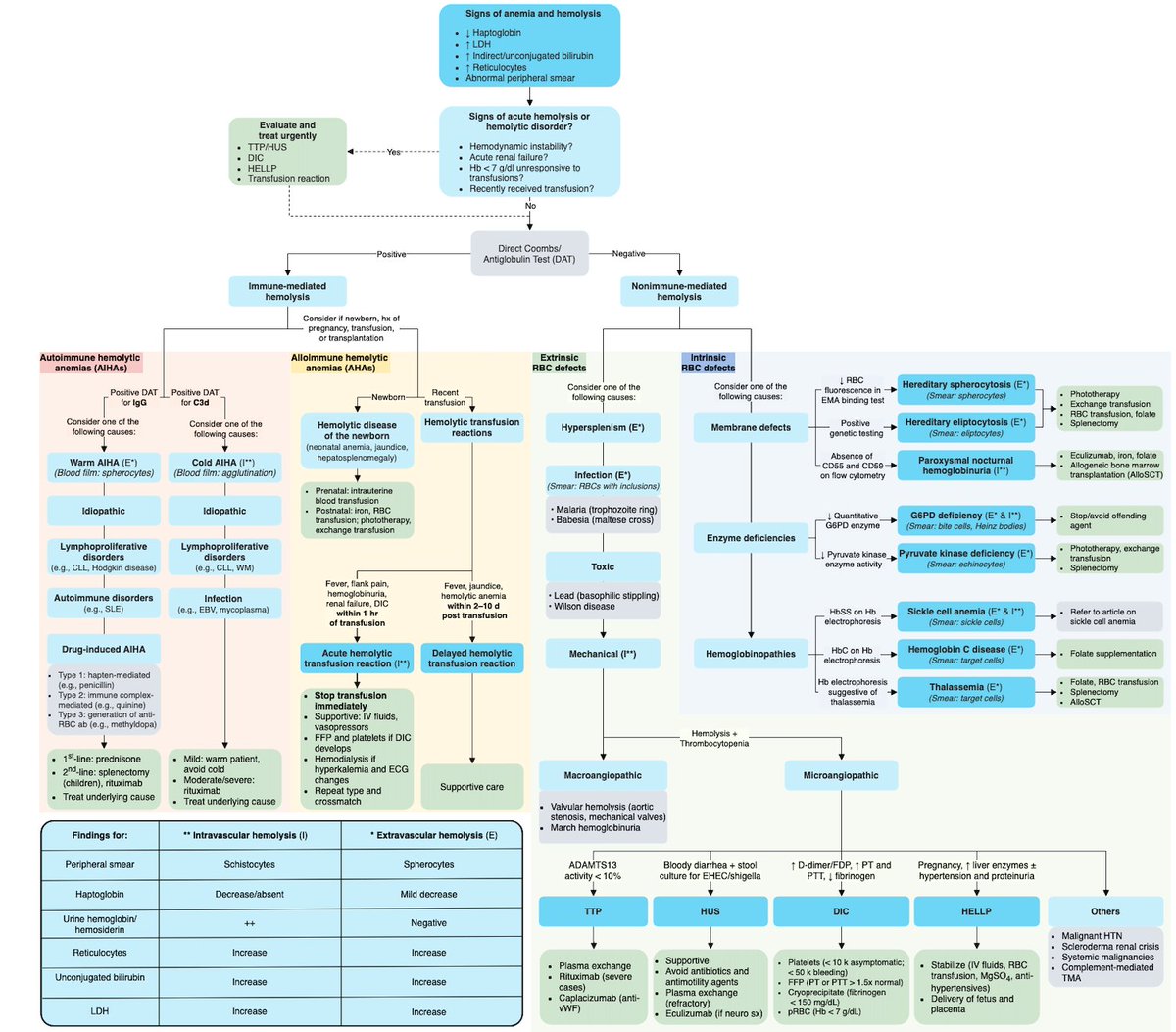
6. Approach to hemolytic anemias
7. Thrombotic Microangiopathies differential
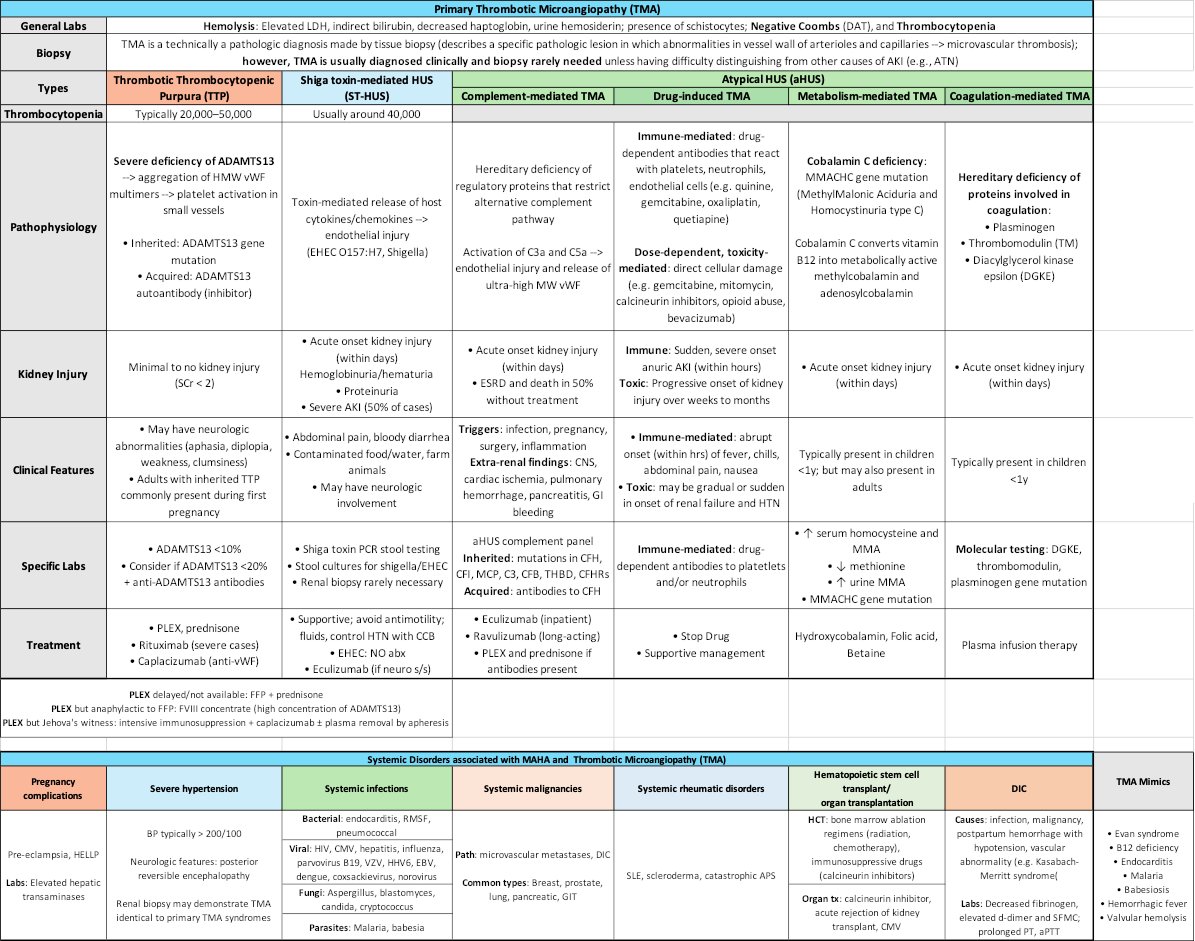
8. Approach to TMA
•PMID: 27497856
•PMID: 29042465
•PMID: 33953366
•PMID: 30504354
•PMID: 27497856
•PMID: 29042465
•PMID: 33953366
•PMID: 30504354

Another pearl. TTP suspected
- No PLEX? --> use FFP (contains ADAMTS13)
- FFP allergy? --> use FVIII concentrate (contains ADAMTS13)
- No PLEX? --> use FFP (contains ADAMTS13)
- FFP allergy? --> use FVIII concentrate (contains ADAMTS13)
• • •
Missing some Tweet in this thread? You can try to
force a refresh