1/ Is Obesity A CHOICE?
The thread 🧵. For starters, please answer the following question ⬇️
The thread 🧵. For starters, please answer the following question ⬇️
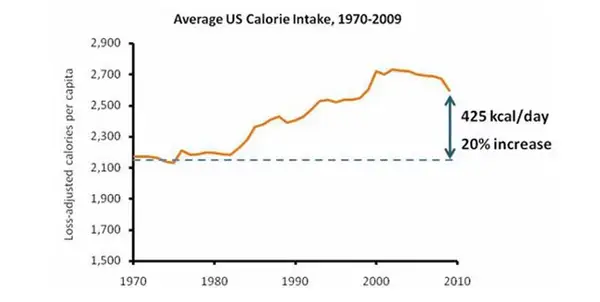
2/ So Why We Are Gaining Weight? Unquestionably, we are eating more, and this increased consumption at a population level is the leading candidate. 

3/ How much more? Around 20% more Calories are ingested per day. With a large % coming from ultra-processed food sources.
aicr.org/resources/blog…
aicr.org/resources/blog…

4/ In fact, @KevinH_PhD's group at the NIH proved that ultra-processed foods lead to increased ad-libitum eating by as much as ~500 Cals per day, which could easily explain the trends in energy intake. pubmed.ncbi.nlm.nih.gov/31105044/

5/ And despite this ultra-processed, ultra-available, ultra-tasty, ultra-convenient, and ultra-marketed food environment, some ppl don't gain wt. Why is that? Bc ~1/2 of your risk of wt gain is related to your inherited genes. Hardly a pre-determined state, but non-trivial.
6/ And while evidence suggests that your biology defends against both weight loss and weight gain, if the environmental pressure imposed by the modern industrial food complex remains at large, the defended weight (or fat mass) will continue to rise.
journals.plos.org/plosbiology/ar…
journals.plos.org/plosbiology/ar…

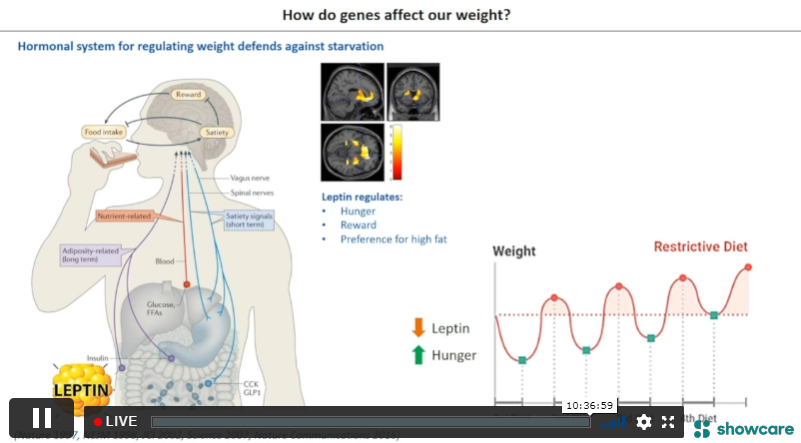
7/ From an evolutionary perspective, this makes sense bc our ancestors had frequent interruptions to their food supply, and therefore the system that monitored energy stores needed to be exquisitely sensitive to promote survival.
8/ During times of shortage, these neural systems would sense the energy deprivation and ⬆️hunger, ⬇️EE, and ⬆️motivation-pleasure from energy-dense foods as means of survival.

9/ It also explains why we are quite sensitive to nudges, advertisements, or any triggers in relation to food during periods of Caloric restriction. It's in our BIOLOGY.
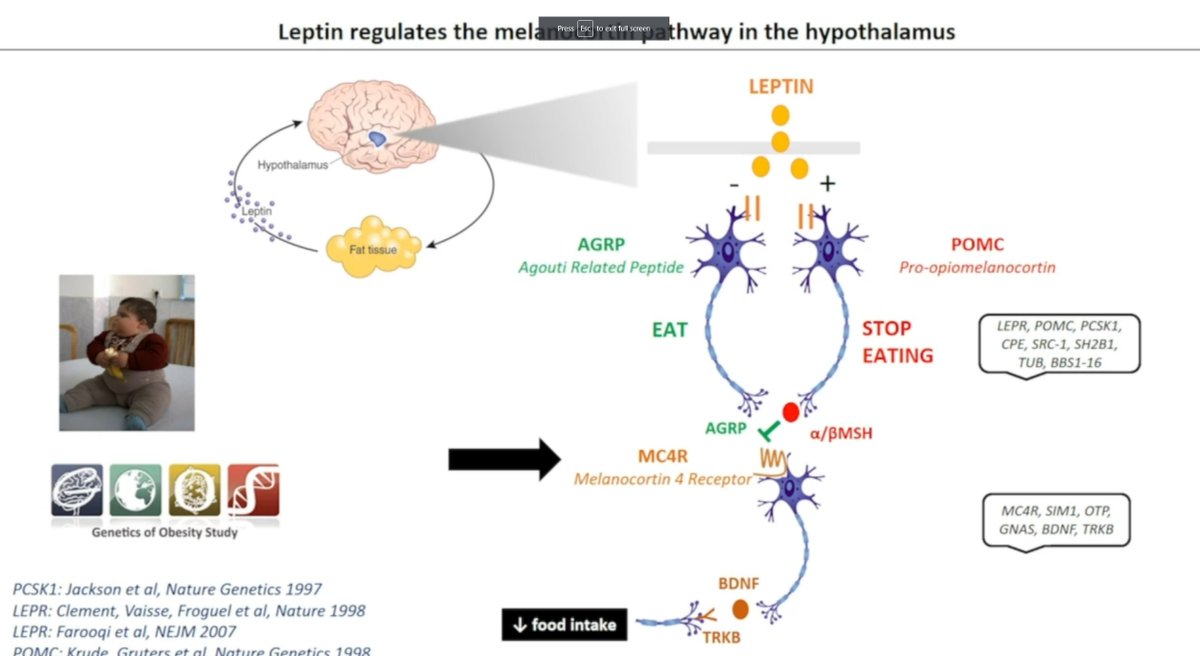
10/ And we actually know that the primary regulator of this system is Leptin, a hormone secreted by adipose tissue in amounts that describe levels of energy stores. See, it's quite an elegant system.
https://twitter.com/MichaelAlbertMD/status/1287476283828404224?s=20&t=GZ2mu7ct9HAzjm6Pl7nHPg
11/ If you want more of an in-depth look at the neural systems involved in obesity, check out a prior thread I made here. ⬇️
https://twitter.com/MichaelAlbertMD/status/1287476268833763329?s=20&t=GZ2mu7ct9HAzjm6Pl7nHPg
12/ Ok, so people can gain weight, with the most prominent drivers being the modern food environment and individual genetic risk, but then what? Why can't people lose weight?
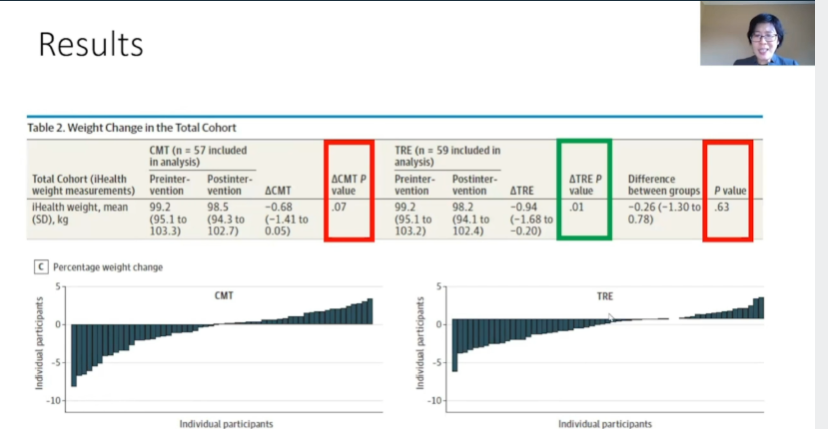
13/ If we look at the data on lifestyle interventions for weight management, 70-90% of people cannot lose a clinically meaningful amount of weight (>10% BW) and maintain that weight loss at 1 year.

14/ This is primarily due to counter-physiological changes that resist wt loss over the long-term (due to our evolutionary biology):
These changes are estimated to be ~100 kcal/d ⬆️increase in appetite and ~25 kcal/d ⬇️ in energy expenditure per kg of body weight lost.
These changes are estimated to be ~100 kcal/d ⬆️increase in appetite and ~25 kcal/d ⬇️ in energy expenditure per kg of body weight lost.

15/ And this counter-physiological mechanism, largely powered by the leptin-melanocortin system to defend our biologically preferred body-weight or fat mass, is why Anderson et al. 2001 observed that 80% of lost weight is regained within 5 years.

16/ Simply, your biology is working against you defend elevated body weights, which is further reinforced by the environment. To lose weight and maintain weight loss, you will have to fight EACH AND EVERY DAY against this system or risk weight relapse.

17/ It's no wonder people struggle to lose weight and keep it off. Unfortunately, your body and the modern world conspire against YOU. It's NOT YOUR FAULT.
18/ So, how do we change this narrative of increasing obesity rates in the US (some predict 50% prevalence by 2030)?

18/ Get back to the root causes: genetics (biology) and environment. While I would love to think we can change the macroenvironment soon, this is likely wishful thinking.
Practical tips (control what you can0:
👉removed UPFs from home
👉talk about these issues as a family
Practical tips (control what you can0:
👉removed UPFs from home
👉talk about these issues as a family
19/ More advanced tips: if you struggle with your weight, consider working with an expert who can help you manage things that are disinhibiting (stress, lack of sleep, mental and emotional despair) and how you can reinforce your good efforts.
20/ Consider working with an Obesity Medicine expert for medication to address biology (the defended elevated body weight/fat mass); this way, your biology is not working against you when you try to lose weight.

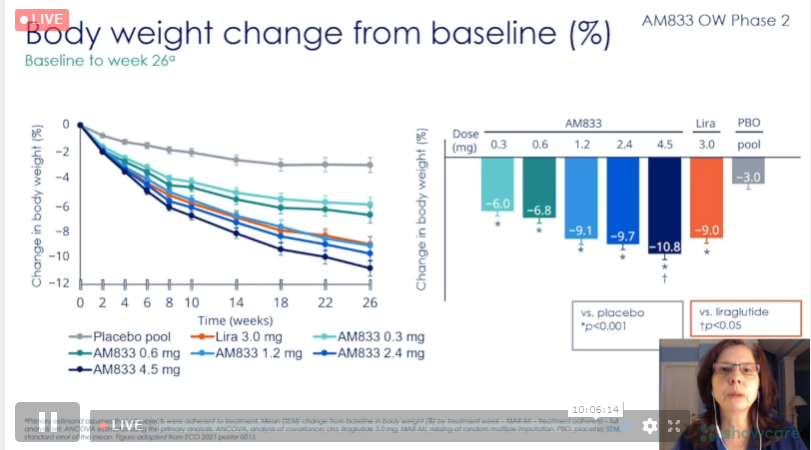
21/ Or for those at risk, bariatric surgery can be life-changing as it remains the only weight loss approach that reliably produces >20% weight loss over years.

21/ Hopefully, this overview makes you question your beliefs around the agency of obesity. As I suspect, some of you may still be unconvinced, and like stonemason hard at work, we will keep whittling away with science bc people living with obesity deserve to be understood. [end]
• • •
Missing some Tweet in this thread? You can try to
force a refresh