Remember that Vitamin C cures sepsis paper that could never be replicated in 9 RCTs?
Turns out there is a good reason why: it’s very likely fraudulent.
More brilliant statistical sleuthing by @K_Sheldrick.
kylesheldrick.blogspot.com/2022/03/eviden…
1/
Turns out there is a good reason why: it’s very likely fraudulent.
More brilliant statistical sleuthing by @K_Sheldrick.
kylesheldrick.blogspot.com/2022/03/eviden…
1/
To understand the proof you should read Dr Sheldricks post.
To summarize, he observed that in this non-randomized study the baseline characteristics of the pre & post intervention groups are far too perfectly matched. This perfect matching is unlikely to occur by chance.
2/
To summarize, he observed that in this non-randomized study the baseline characteristics of the pre & post intervention groups are far too perfectly matched. This perfect matching is unlikely to occur by chance.
2/


Specifically, you’d expect to see a range of p values for each baseline characteristic.
(This is especially true in a tiny trial with only n=47 patients)
Instead the range of p values for almost every variable was exactly 1.
This is *extremely* unlikely to occur by chance.
3/
(This is especially true in a tiny trial with only n=47 patients)
Instead the range of p values for almost every variable was exactly 1.
This is *extremely* unlikely to occur by chance.
3/


It’s also worth considering the context.
After the Marik paper was published in CHEST in 2017, many RCTs were launched to validate it.
Every single RCT of vitamin C in sepsis (9 of them) was negative.
No one has *ever* replicated Marik’s finding.
onepagericu.com/blog/a-skeptic…
4/
After the Marik paper was published in CHEST in 2017, many RCTs were launched to validate it.
Every single RCT of vitamin C in sepsis (9 of them) was negative.
No one has *ever* replicated Marik’s finding.
onepagericu.com/blog/a-skeptic…
4/
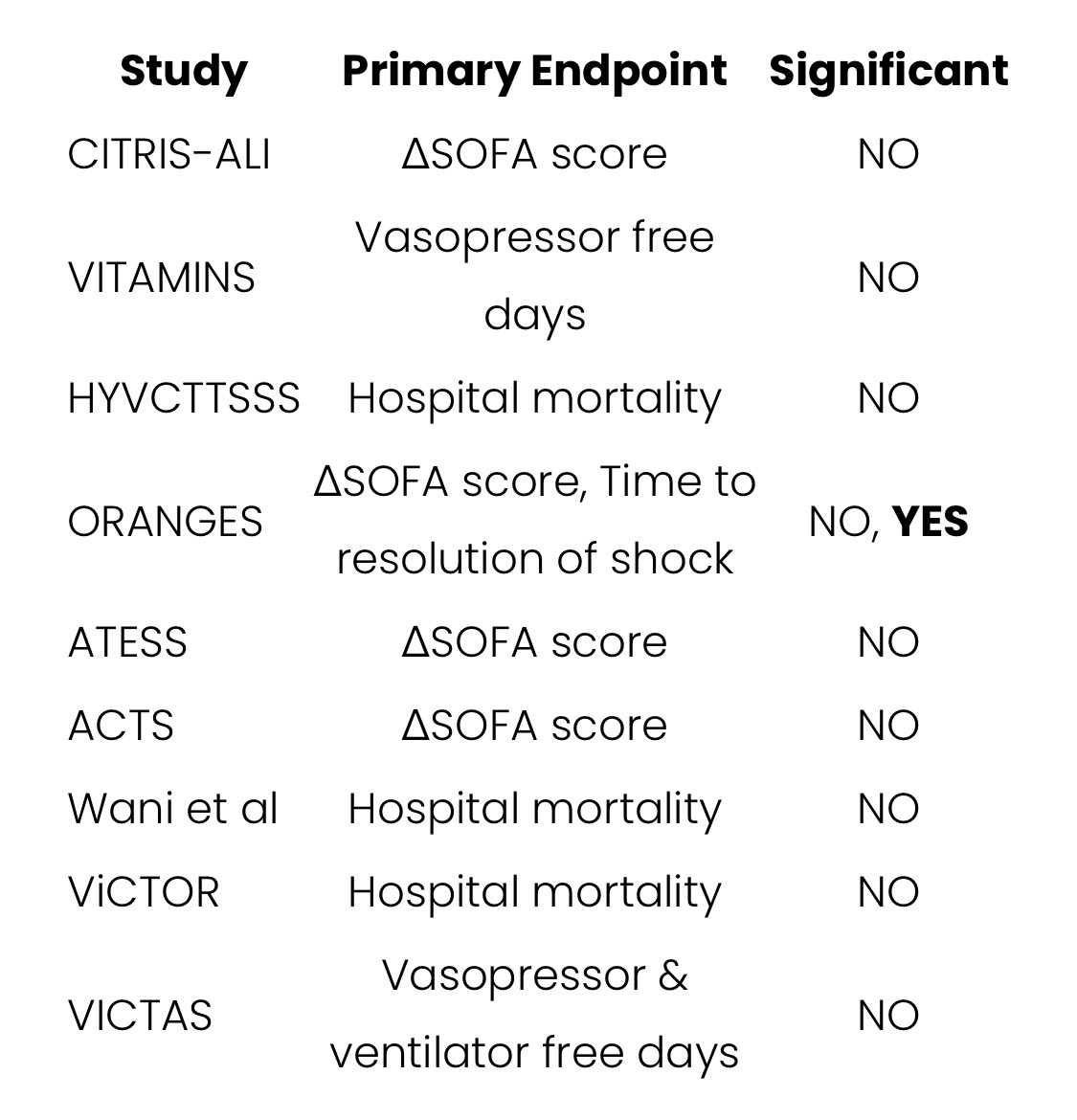



Not only has the Marik vitamin C in sepsis work *NEVER* been replicated, but as more high quality studies were completed the trend towards null has become obvious:
5/
5/

As I pointed out in 2020, Marik’s trial of a “metabolic cocktail for sepsis” was truly an outlier:
onepagericu.com/blog/a-skeptic…
6/
onepagericu.com/blog/a-skeptic…
6/

The other important context happened more recently.
Marik, Kory, & Co authored a paper about ivermectin that (like the vitamin C paper 3 years earlier) claimed an improbably huge mortality reduction.
This paper turned out to be based on incorrect data. It was retracted.
7/
Marik, Kory, & Co authored a paper about ivermectin that (like the vitamin C paper 3 years earlier) claimed an improbably huge mortality reduction.
This paper turned out to be based on incorrect data. It was retracted.
7/
https://twitter.com/nickmmark/status/1458627706262675458
Some details are still murky, but Marik’s career appears to have ended ignominiously:
In November his clinical privileges were suspended.
He sued his employer demanding the right to prescribe vitamin C & ivermectin. He lost this lawsuit & resigned in December.
A sad end
8/
In November his clinical privileges were suspended.
He sued his employer demanding the right to prescribe vitamin C & ivermectin. He lost this lawsuit & resigned in December.
A sad end
8/
‘That ends this strange eventful history’ of Vitamin C in Sepsis.
What can we learn from this sad saga?
1. Remember that extraordinary claims require extraordinary evidence.
As a profession we need to remain skeptical of extraordinary claims. Especially when the study’s n=47.
9/
What can we learn from this sad saga?
1. Remember that extraordinary claims require extraordinary evidence.
As a profession we need to remain skeptical of extraordinary claims. Especially when the study’s n=47.
9/
https://twitter.com/nickmmark/status/1391056442245849090
2. It’s ok to be an “early adopter” but you need to “de-adopt” quickly too.
If you jump on the new therapy bandwagon be ready to jump off when the first RCTs are negative.
This took way too long.
10/
If you jump on the new therapy bandwagon be ready to jump off when the first RCTs are negative.
This took way too long.
10/
https://twitter.com/nickmmark/status/1218176953821171713
3. Be weary of “eminence based medicine”
If a claim only seems plausible because of who’s making it, it probably isn’t plausible.
Correlary: if “only someone so famous could have published this” it probably shouldn’t have been published. (Cough Ahem Ioannidis cough)
11/
If a claim only seems plausible because of who’s making it, it probably isn’t plausible.
Correlary: if “only someone so famous could have published this” it probably shouldn’t have been published. (Cough Ahem Ioannidis cough)
11/
4. Scrutinize table 1 & don’t be afraid to double check stats yourself
We need more post hoc peer review. Checking stats is a great way to learn & catch errors
My friend @drlessing taught me that a good journal club can easily become a letter to the editor. #TipForNewDocs
12/
We need more post hoc peer review. Checking stats is a great way to learn & catch errors
My friend @drlessing taught me that a good journal club can easily become a letter to the editor. #TipForNewDocs
12/
And finally
5. New therapies require SAFETY and EFFICACY
Just because a therapy is likely safe doesn’t mean we get to skip proving efficacy.
A harmless ineffective therapy isn’t tantamount to a safe beneficial one.
(It’s truly surprising how many people don’t understand this)
13/
5. New therapies require SAFETY and EFFICACY
Just because a therapy is likely safe doesn’t mean we get to skip proving efficacy.
A harmless ineffective therapy isn’t tantamount to a safe beneficial one.
(It’s truly surprising how many people don’t understand this)
13/
If you are wondering about the harms of a “totally harmless vitamin” consider:
- IV VitC isn’t cheap (~$500)
- giving 500 mLs of unnecessary IVF daily probably isn’t benign
- rarely patients can have serious allergic reactions to the preservatives in a bag of IV vitC
14/
- IV VitC isn’t cheap (~$500)
- giving 500 mLs of unnecessary IVF daily probably isn’t benign
- rarely patients can have serious allergic reactions to the preservatives in a bag of IV vitC
14/
Also consider the opportunity costs of ineffective therapies like VitC:
- 10s of millions of dollars were spent on the 9 RCTs disproving “the metabolic cure for sepsis”. We could have spent that money for better developing new *effective* therapies for sepsis.
15/
- 10s of millions of dollars were spent on the 9 RCTs disproving “the metabolic cure for sepsis”. We could have spent that money for better developing new *effective* therapies for sepsis.
15/
Lastly, think how confusing this can be for laypersons. Look at these 2 headlines👇
Medicine changes as science evolves, but every high profile “medical reversal” may undermine the public’s faith in science/medicine. It behooves us to avoid hyperbolic talk of “cures”
16/
Medicine changes as science evolves, but every high profile “medical reversal” may undermine the public’s faith in science/medicine. It behooves us to avoid hyperbolic talk of “cures”
16/


• • •
Missing some Tweet in this thread? You can try to
force a refresh