Now to talk about Phosphatonins and #phosphorus metabolism/bone disease by Dr. Kumar moderated by @sfeirjad...I'm ready to learn since admittedly I know little of this #AACE2022 #Endotwitter #bone 

Why bother about phosphorus? Well it plays many roles in cellular signaling and maintenance of membrane structure of #bone. Low concentrations associated with rhabdo, decreased cardiac function and bone dysfunction (#osteomalacia, #rickets). low and high phos causes bone disease


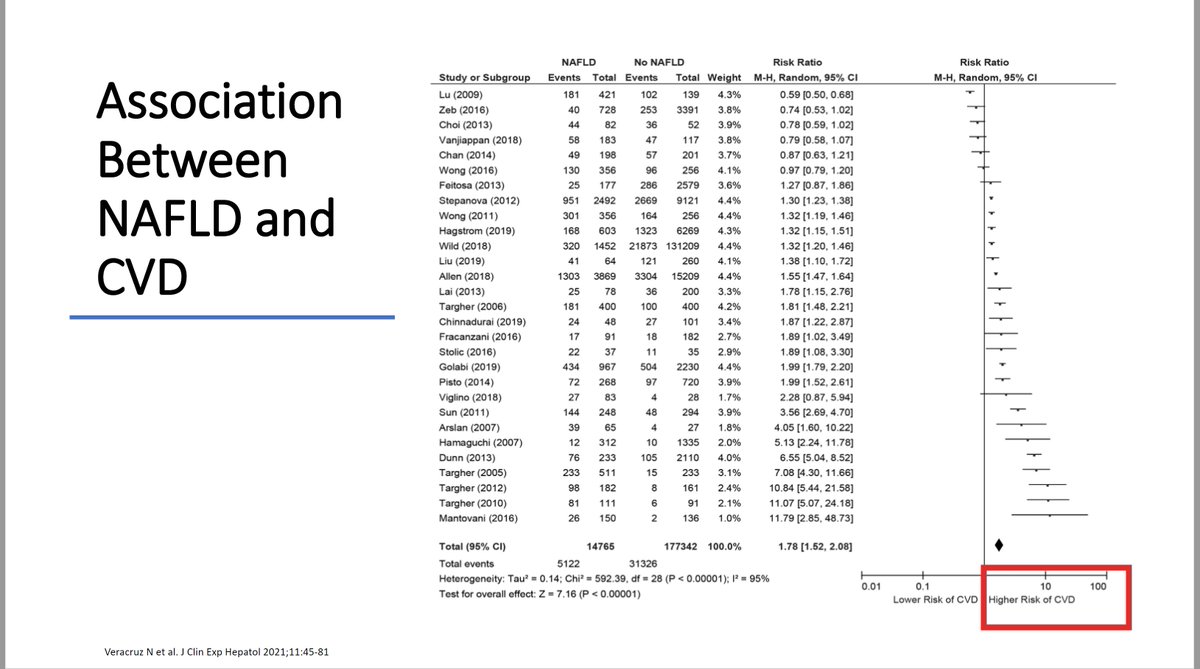
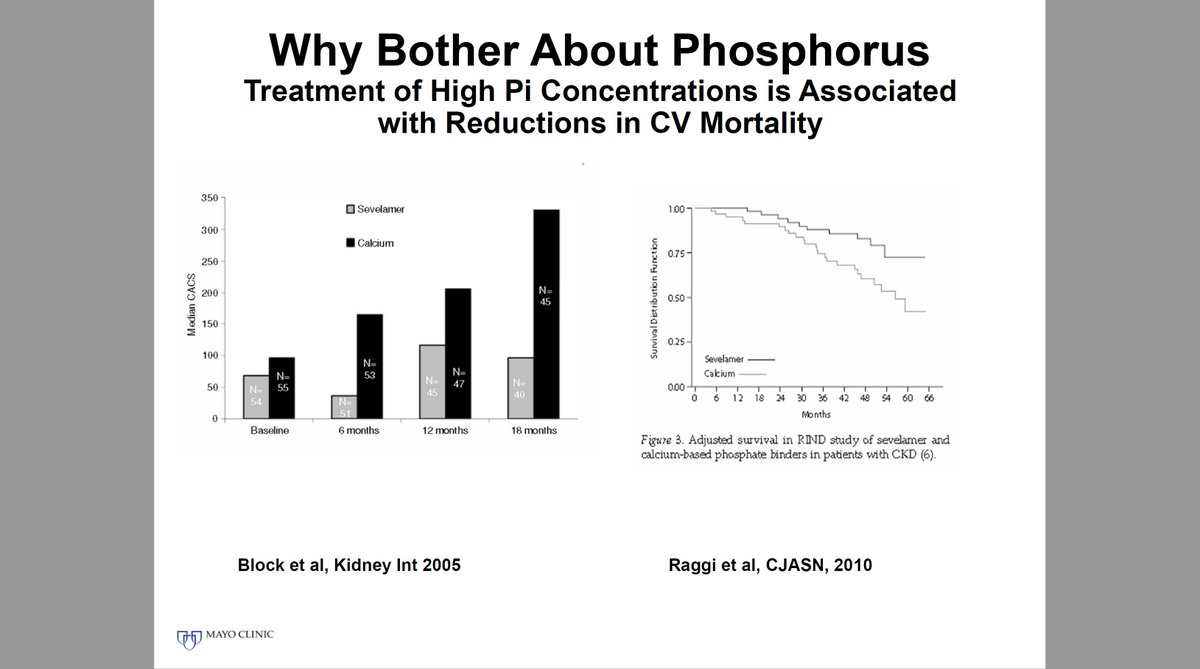
High Phos Concentrations are Associated with CV Disease and Excess Mortality in CRF and decreasing levels reduces CV mortality

There are many different regulators to phos homeostasis. Not surprisingly since we are talking endo & bone here, there are many impt players to help maintain normal serum phosphate levels especially in dietary phos


What are causes of #hypophosphatemia, there are many

What is a phosphatonin? -- my exact question when I saw the lecture title -- factors that play a role in phosphate homeostasis -- common one we know is FGF-23


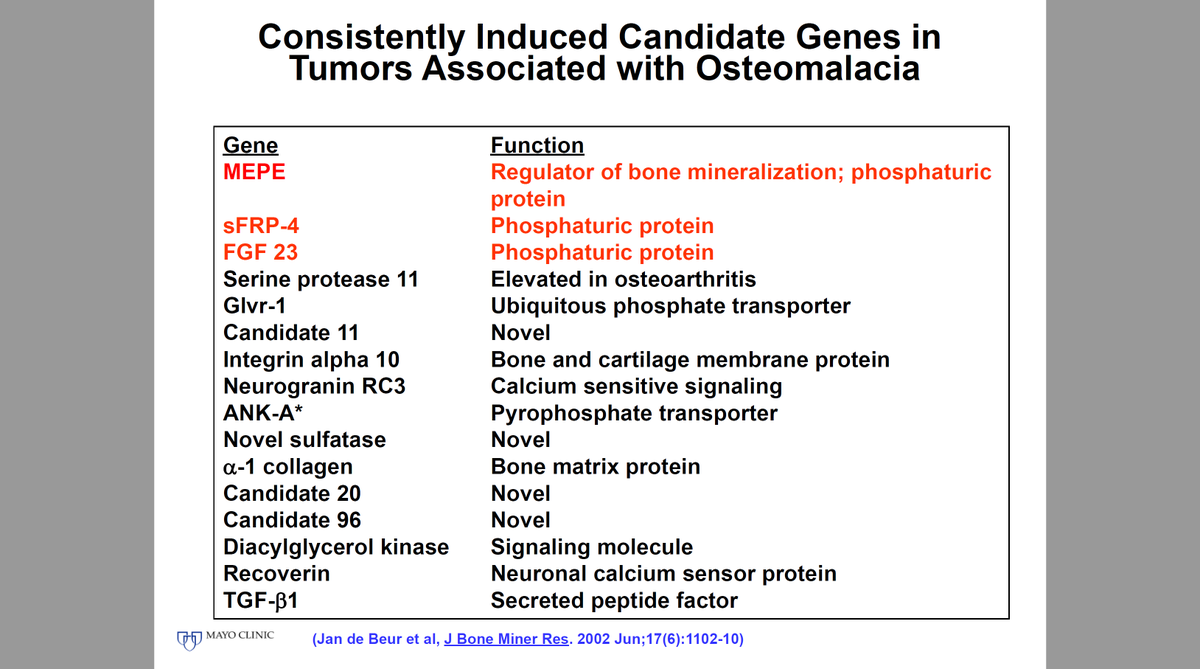
The phosphatonins FGF-23 and sFRP-4 reduce renal phos reabsorption By reducing the number of Na-Pi IIa
transporters on the surface of renal tubular
epithelial cells
transporters on the surface of renal tubular
epithelial cells

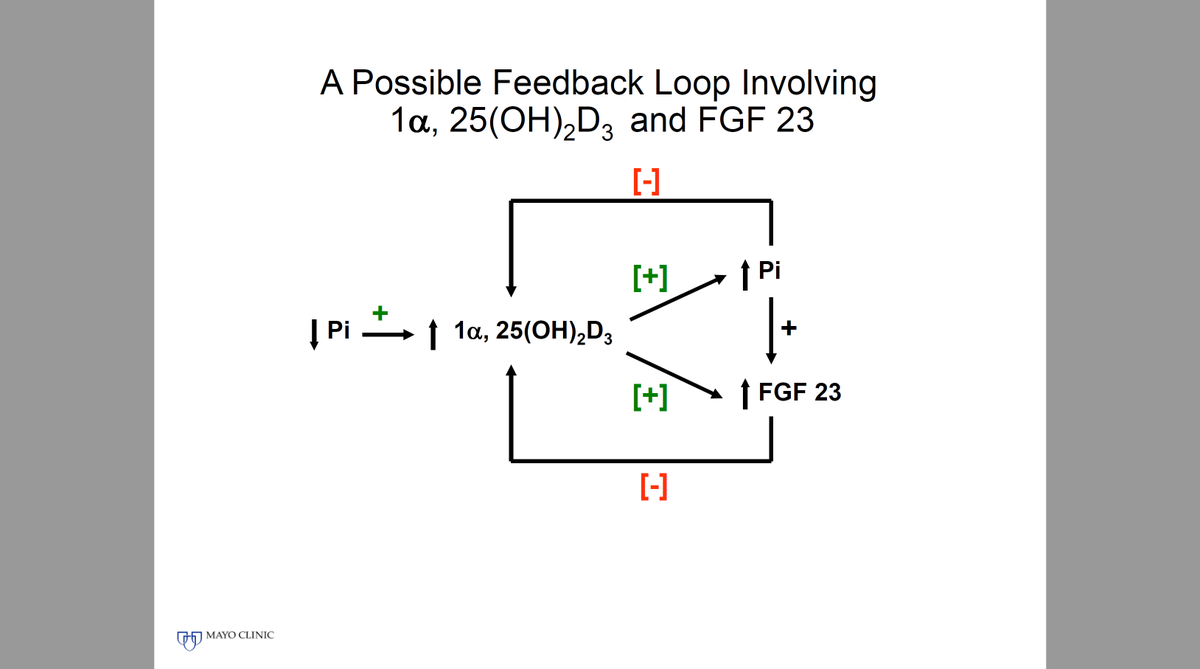
The Phosphatonins FGF-23, sFRP-4 and FGF-7 Reduce 1α, 25- Dihydroxyvitamin D Production by
Inhibiting the 25-Hydroxyvitamin D 1α-Hydroxylase --- there is a feedback loop
Inhibiting the 25-Hydroxyvitamin D 1α-Hydroxylase --- there is a feedback loop
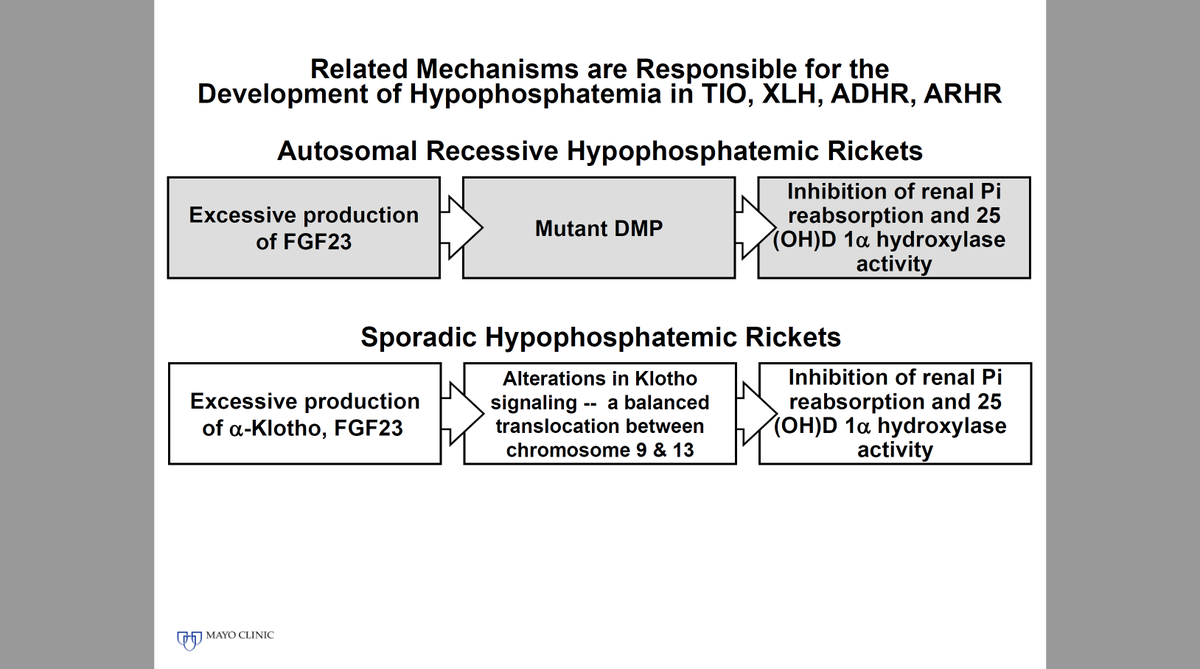
Why do we care? Well it's b/c when there is too much phosphatonin activity you get hypophosphatemia and bone disease (TIO, XLH, ADHR, renal failure etc)


The opposite (hyperphosphatemia) happens when you don't have enough phosphatonin activity

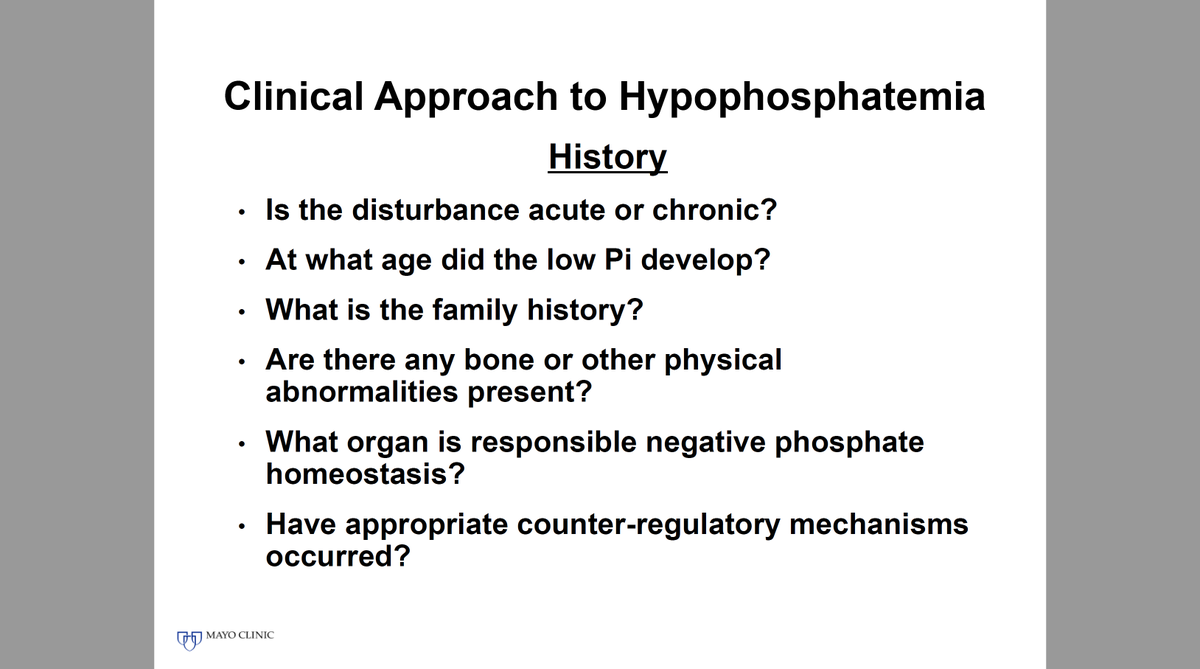
Now how to use this clinically? History is impt and lab evaluation -- refer to the third slide attached below as it is a great reference on expected lab changes in different hypophosphatemic conditions


• • •
Missing some Tweet in this thread? You can try to
force a refresh