
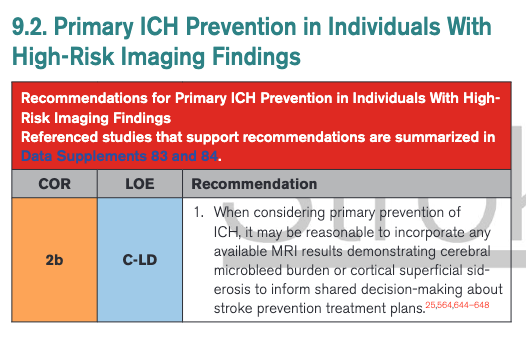
re: ICH Prevention in People w ⬆️Risk MRI findings in @American_Heart updated 2022 ICH guidelines🧠🩸
📌 Refers to incidentally found MRI markers of small vessel disease (SVD) - a common question
Prompted by @interneurona unpacking below (short 🪀)
📌 Refers to incidentally found MRI markers of small vessel disease (SVD) - a common question
Prompted by @interneurona unpacking below (short 🪀)
https://twitter.com/interneurona/status/1526578646680494081
For context:
🚫MRI is not routinely done for risk stratification of first-ever spontaneous ICH risk
🔮MRI is occasionally available in certain people/pts w/o ICH: may show SVD markers concerning for future ICH risk
〽️These markers are: microbleeds, superficial siderosis
1/
🚫MRI is not routinely done for risk stratification of first-ever spontaneous ICH risk
🔮MRI is occasionally available in certain people/pts w/o ICH: may show SVD markers concerning for future ICH risk
〽️These markers are: microbleeds, superficial siderosis
1/
The populations that this might be relevant to are:
- healthy elderly
- ischemic stroke
- memory clinic
- any pt who got a brain MRI for a different indication (e.g. migraines)
- non-ICH cerebral amyloid angiopathy (CAA)
#neuroradiology #Alzheimers #stroke
2/
- healthy elderly
- ischemic stroke
- memory clinic
- any pt who got a brain MRI for a different indication (e.g. migraines)
- non-ICH cerebral amyloid angiopathy (CAA)
#neuroradiology #Alzheimers #stroke
2/
As the guidelines point-out:
🤏🏿little data exist from these populations around the Q
But there are some important "guiding principles" 🚢, a "thought process" that clinicians may use.
(I will go beyond wha's covered in the @American_Heart updated 2022 ICH guidelines🧠🩸)
3/
🤏🏿little data exist from these populations around the Q
But there are some important "guiding principles" 🚢, a "thought process" that clinicians may use.
(I will go beyond wha's covered in the @American_Heart updated 2022 ICH guidelines🧠🩸)
3/
Thought process:
In general, absolute risk of first-ever ICH:
-⬇️⬇️⬇️ much lower than recurrent ICH risk
-much less than ischemic stroke risk in the same patient
✨These hold, even in the presence MRI SVD markers @microbleeds
4/
In general, absolute risk of first-ever ICH:
-⬇️⬇️⬇️ much lower than recurrent ICH risk
-much less than ischemic stroke risk in the same patient
✨These hold, even in the presence MRI SVD markers @microbleeds
4/
Thought process cont'd:
📰Literature over the years disproportionately emphasized that CMBs increase ICH risk.
⚡️This is not true!
👁🗨CMBs are associated w ⬆️HR for ICH, but absolute ischemic stroke risk always >>> ICH risk
(see👇🏿in ischemic stroke where this is relevant)
/5
📰Literature over the years disproportionately emphasized that CMBs increase ICH risk.
⚡️This is not true!
👁🗨CMBs are associated w ⬆️HR for ICH, but absolute ischemic stroke risk always >>> ICH risk
(see👇🏿in ischemic stroke where this is relevant)
/5

Thought process cont'd:
-CMBs also increase ischemic stroke risk, since they are related w vascular risk factors (especially mixed and deep ones)
-Even in symptomatic CAA, lobar CMBs are not associated with ICH risk when you control for cSS
6/
-CMBs also increase ischemic stroke risk, since they are related w vascular risk factors (especially mixed and deep ones)
-Even in symptomatic CAA, lobar CMBs are not associated with ICH risk when you control for cSS
6/

To wrap up re CMBs and prevention of first ever ICH:
-CMBs should be viewed as more general markers of stroke risk (both ischemic and ICH)
-When incidental, they should not affect decision against antithrombotics💊 when there is a proper indication (e.g. DAPT in stroke)
7/
-CMBs should be viewed as more general markers of stroke risk (both ischemic and ICH)
-When incidental, they should not affect decision against antithrombotics💊 when there is a proper indication (e.g. DAPT in stroke)
7/
Would a #Tweetorial on microbleeds' clinical relevance in stroke be of interest?
I thought most questions were sorted in the field, but still related issues come up all the time! @MicieliA_MD @nbavar @ShadiYaghi2 @WorldStrokeEd @caseyalbin
I thought most questions were sorted in the field, but still related issues come up all the time! @MicieliA_MD @nbavar @ShadiYaghi2 @WorldStrokeEd @caseyalbin
🎢cSS, unlike CMBs, is a "hardcore" hemorrhagic marker strongly associated w CAA-bleeding 🩸🧠
cSS is extremely rare in the general population and ischemic stroke/TIA (~1%), so less of a clinical dilemma
8/
cSS is extremely rare in the general population and ischemic stroke/TIA (~1%), so less of a clinical dilemma
https://twitter.com/a_charidimou/status/1098985496041136128?s=20&t=AjnGjjlNBPcPrkGPYvvSpA
https://twitter.com/MicieliA_MD/status/1520866017324322817?s=20&t=AjnGjjlNBPcPrkGPYvvSpA
8/
@interneurona: I think the brief section on "Primary ICH Prevention in Individuals With High-Risk Imaging" in the updated 2022 ICH guidelines is an excellent addition.
But only provides little practical guidance for the clinician (that's guidelines' nature in the absence of evidence). Looking at available data critically and synthetically provides a framework, as I tried to summarise in this 🧵
#neurotwitter #NeuroTwitter #NeuroRad #Neurology
#neurotwitter #NeuroTwitter #NeuroRad #Neurology
• • •
Missing some Tweet in this thread? You can try to
force a refresh




