
Pay attention to this thread:
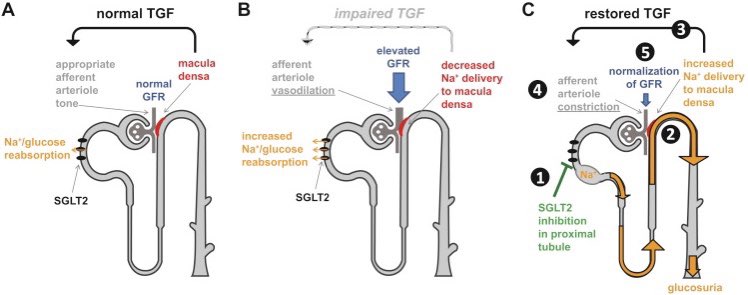
Sodium/Glucose Cotransporter *2* (SGLT2) receptors are in the *1st* part of the proximal tubule, where 90% of glucose reabsorption occurs & also where SGLT2 inhibitors like empagliflozin work.
SGLT *1* receptors are in the *2nd* part of the tubule.
Sodium/Glucose Cotransporter *2* (SGLT2) receptors are in the *1st* part of the proximal tubule, where 90% of glucose reabsorption occurs & also where SGLT2 inhibitors like empagliflozin work.
SGLT *1* receptors are in the *2nd* part of the tubule.

SGLT2i ↓ systolic HF mortality in patients with OR without diabetes.
Drugs that ↓ systolic HF mortality:
•ß-blockers (metoprolol, bisoprolol, carvedilol)
•ACEi
•ARBs
•MRAs
•Hydralazine (with nitrates)
•Neprelysin inhibitor (sacubitril)
•SGLT2 inhibitors
Drugs that ↓ systolic HF mortality:
•ß-blockers (metoprolol, bisoprolol, carvedilol)
•ACEi
•ARBs
•MRAs
•Hydralazine (with nitrates)
•Neprelysin inhibitor (sacubitril)
•SGLT2 inhibitors
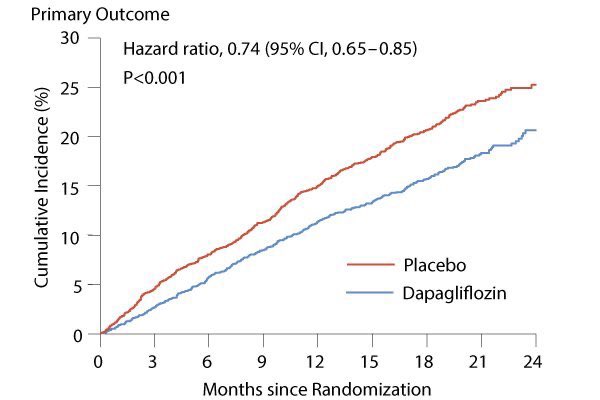
Additionally, SGLT2 inhibitors ↑ sodium delivery to macula densa and SLOW the progression of GFR decline in kidney disease by restoring the tubuloglomerular feedback (TGF) and are associated with DECREASED mortality from kidney disease among patients with diabetes.

Inhibition of SGLT2 is also associated with ↑ Mg level. How?
Three mechanisms:
↓ insulin secretion = ↓ Mg excretion
↑ glucagon release = ↑ Mg reabsorption
↓ vascular volume = RAAS activation = ↑ Mg reabsorption
Three mechanisms:
↓ insulin secretion = ↓ Mg excretion
↑ glucagon release = ↑ Mg reabsorption
↓ vascular volume = RAAS activation = ↑ Mg reabsorption

The most common (and significant) side effect of SGLT2 inhibitors is genital yeast infections.
The “black box” label of amputations associated with SGLT2 inhibitors has been REMOVED by the FDA. It is NO LONGER the right answer on your test.
fda.gov/media/141533/d…
The “black box” label of amputations associated with SGLT2 inhibitors has been REMOVED by the FDA. It is NO LONGER the right answer on your test.
fda.gov/media/141533/d…
SGLT2 inhibitors are also associated with euglycemic ketoacidosis. That is why these drugs should be temporarily STOPPED before surgery.
This is the single most significant step that most of you will forget on the #USMLE.
This is the single most significant step that most of you will forget on the #USMLE.
By themselves, SGLT2i do not cause significant hypoglycemia. But if a T2DM patient is on both insulin and SGLT2i, the risk of hypoglycemia increases.
In this case, we reduce the dose of the SGLT2 inhibitor (not the basal insulin).
In this case, we reduce the dose of the SGLT2 inhibitor (not the basal insulin).
For DIASTOLIC heart failure, SGLT2 inhibitors decrease disease exacerbations and hospitalizations. But unlike SYSTOLIC heart failure, their effect on mortality is UNCLEAR.
#USMLE has a plethora of topics to test you on. It will not engage in things that are not 1,000% clear.
#USMLE has a plethora of topics to test you on. It will not engage in things that are not 1,000% clear.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



