1/Mass shootings are a great tragedy. Commentators often casually link them w/mental illness. But are there neuro imaging findings to correlate w/their behavior?
A nonpolitical 🧵about what we can see in brains of mass killers
#neuroscience #MedTwitter #NeuroTwitter #GunViolence
A nonpolitical 🧵about what we can see in brains of mass killers
#neuroscience #MedTwitter #NeuroTwitter #GunViolence
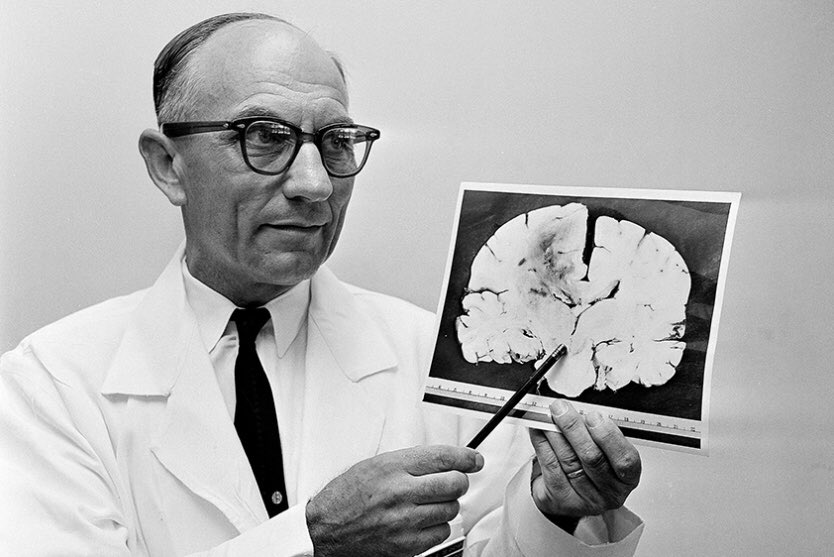
2/The first mass killer was Charles Whitman, the bell tower shooter in 1966. He complained of headaches before the shooting & a glioblastoma was found in his frontal lobe, leading people to believe that structural abnormalities may lead to this behavior.
thedailytexan.com/2016/07/30/fif…
thedailytexan.com/2016/07/30/fif…
3/Unfortunately, this theory did not hold. No other mass killer has had a structural lesion like a tumor. It is often difficult to draw conclusions since much of the brain tissue in these killers is often destroyed by either self or non self inflicted wounds to the head at death
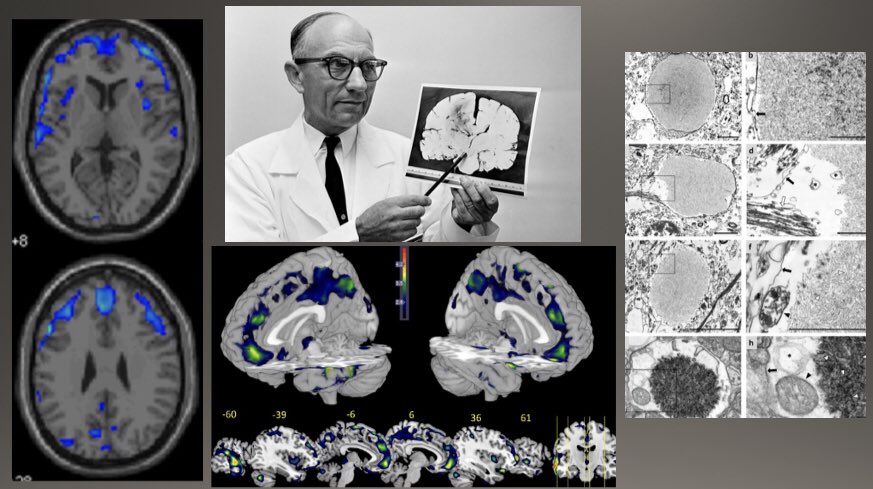
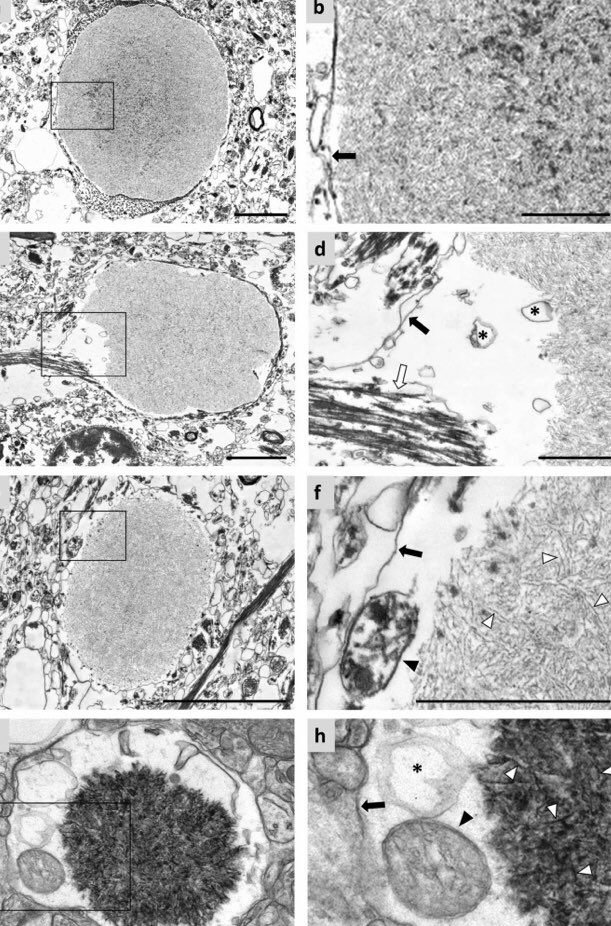
4/Despite this, autopsy in Las Vegas shooter Stephen Paddock showed ⬆️ corpora amylacea, a cellular debris product seen in aging, in his frontal lobe(impulse control) & hippocampus (memory). However, he had no neurodegeneration
nytimes.com/2018/02/09/us/…
nature.com/articles/s4159…
nytimes.com/2018/02/09/us/…
nature.com/articles/s4159…
4/Also, b/c of the small number of mass killings relative to general homicides, it is difficult to draw sweeping conclusions. Therefore, people have tried to look for differences in brains of people who commit homicide vs those who commit other violent offenses to look for clues
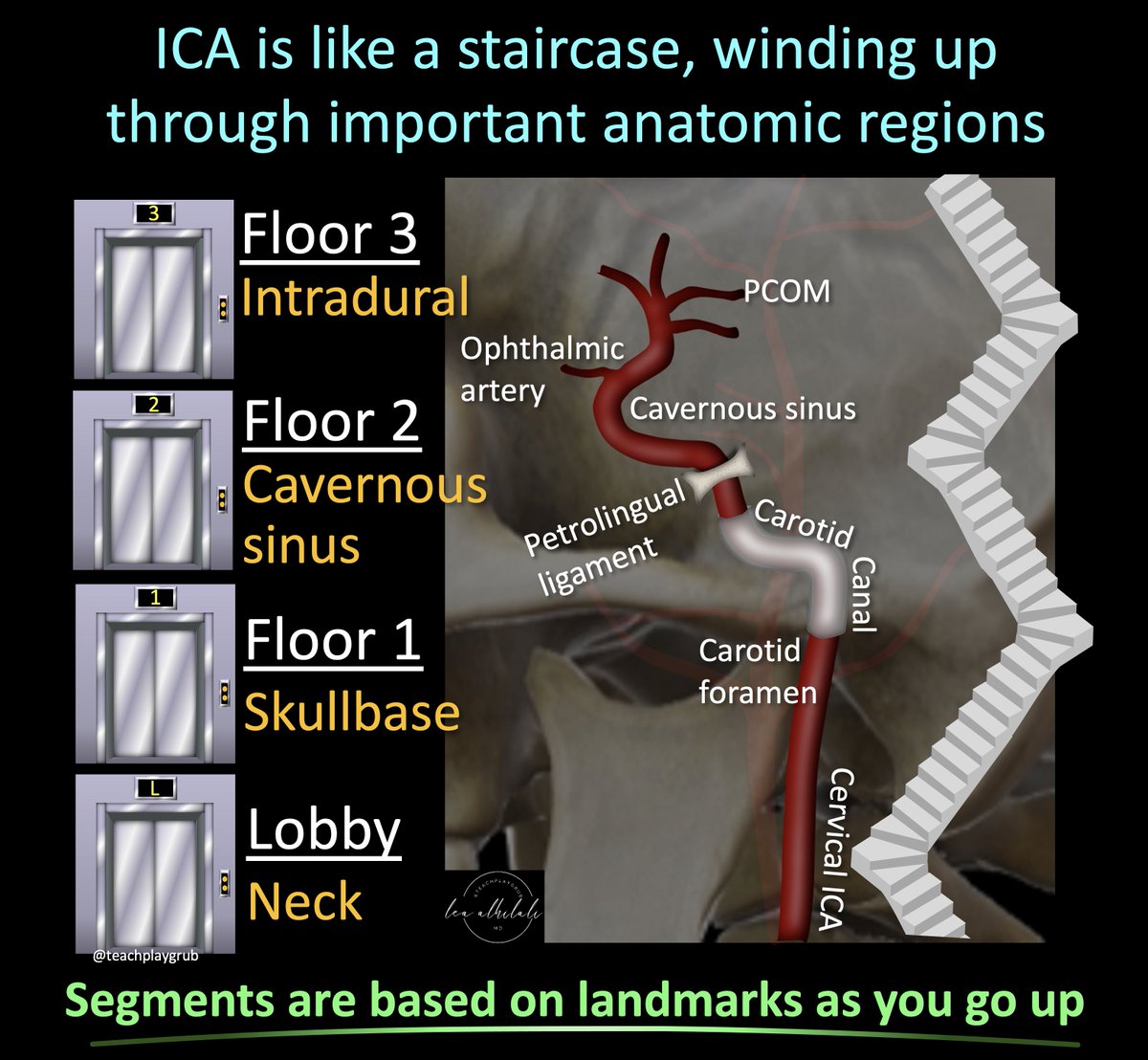
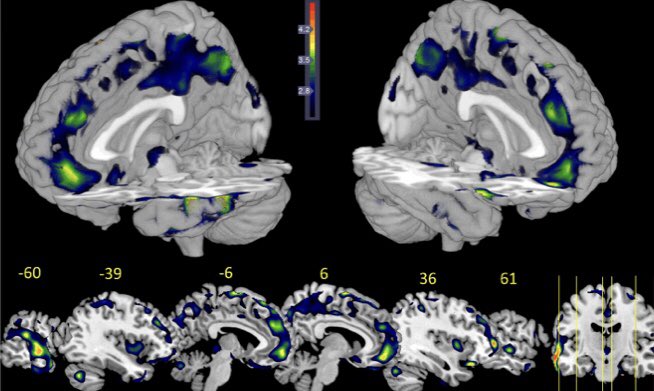
5/Studies have found decreased gray matter (neurons) in the frontal and temporal regions in those who commit homicide compared to other violent offenders, the same regions of accelerated aging changes in the Las Vegas shooter.
documentcloud.org/documents/6428…
documentcloud.org/documents/6428…
6/Unfortunately, however, there is no smoking gun on imaging that can alert us to the people who may commit these heinous acts or help us to understand why they committed them. They will, sadly, remain a tragic mystery.
• • •
Missing some Tweet in this thread? You can try to
force a refresh