
Once again there is a wave of #misinformation about #ExcessMortality & #vaccines in the US.
A mysterious insurance report says “excess mortality is rising” could it be the vaccines?
No. Virtually all the excess mortality is associated with COVID infections!
A debunking 🧵.
1/
A mysterious insurance report says “excess mortality is rising” could it be the vaccines?
No. Virtually all the excess mortality is associated with COVID infections!
A debunking 🧵.
1/



Every few months, a myth of “unexplained deaths not from COVID” resurfaces.
Last time they claimed “young people” were inexplicably dying. Looking at the actual data it was pretty clear that virtually all the excess deaths under 45 were due to COVID.
2/
Last time they claimed “young people” were inexplicably dying. Looking at the actual data it was pretty clear that virtually all the excess deaths under 45 were due to COVID.
https://twitter.com/nickmmark/status/1452487179364564996?s=20&t=Ub8btz0TcqDi3OYx3UKtiw
2/
In a later incarnation, this conspiracy theory revolved around a mysterious (and nameless) "insurance industry expert” & "former Wall Street analyst” who did his own analysis and “found an 84% increase in excess mortality."
This too has been debunked.
reuters.com/article/factch…
3/
This too has been debunked.
reuters.com/article/factch…
3/
Let’s look at the actual data:
If we look at weekly deaths of all cause, we can see five spikes above baseline in weekly deaths, each corresponding to a wave of the pandemic.
Source: CDC
cdc.gov/nchs/nvss/vsrr…
4/
If we look at weekly deaths of all cause, we can see five spikes above baseline in weekly deaths, each corresponding to a wave of the pandemic.
Source: CDC
cdc.gov/nchs/nvss/vsrr…
4/

How much of the increase in mortality is due to COVID?
If we look at # of deaths/week, comparing weekly COVID deaths to total deaths. we can see the answer is almost all of it!
Example: Of the ~27k excess deaths in early 2021, ~26k were due to COVID!
cdc.gov/nchs/nvss/vsrr…
5/
If we look at # of deaths/week, comparing weekly COVID deaths to total deaths. we can see the answer is almost all of it!
Example: Of the ~27k excess deaths in early 2021, ~26k were due to COVID!
cdc.gov/nchs/nvss/vsrr…
5/




But we don’t have to look just at correlations, because Doctors put the cause of death on death certificates.
Looking at COVID associated deaths🟦vs non COVID deaths 🟩, we can see that virtually all of the excess mortality can been attributed to COVID infection!
Source: CDC
6/
Looking at COVID associated deaths🟦vs non COVID deaths 🟩, we can see that virtually all of the excess mortality can been attributed to COVID infection!
Source: CDC
6/

This isn’t really surprising since COVID was the THIRD leading cause of death in the US in 2021.
cdc.gov/mmwr/volumes/7…
7/
cdc.gov/mmwr/volumes/7…
7/
Not only do mortality spikes correlate with surges in COVID infections, they do NOT correlate with vaccinations.
Compare 3 lines: weekly excess Mortality ⬛, COVID cases 🟥, & vaccinations🟦
The correlation (R²) is higher for mortality⬛ & cases🟥.
github.com/hmatejx/COVID_…
8/
Compare 3 lines: weekly excess Mortality ⬛, COVID cases 🟥, & vaccinations🟦
The correlation (R²) is higher for mortality⬛ & cases🟥.
github.com/hmatejx/COVID_…
8/


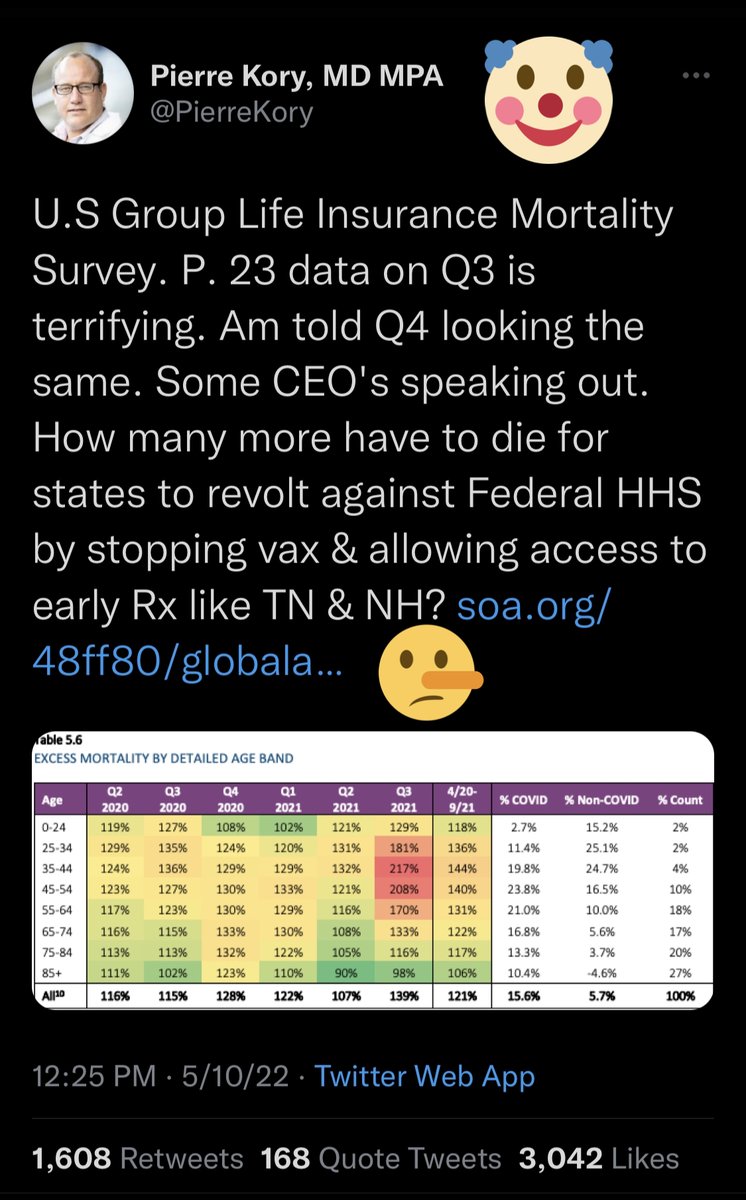
If we look at that insurance report that Kory shared (and clearly didn’t read), we can see more evidence that vaccination *reduces* excess mortality.
Specifically excess mortality is HIGHEST in the places with the LOWEST vaccinations!
Source: soa.org/48ff80/globala…
9/
Specifically excess mortality is HIGHEST in the places with the LOWEST vaccinations!
Source: soa.org/48ff80/globala…
9/

This too isn't surprising, we know that at this point in the pandemic the vast majority of COVID mortality occurs among unvaccinated people.
Source: Our World in Data
ourworldindata.org/grapher/united…
10/
Source: Our World in Data
ourworldindata.org/grapher/united…
10/

Summary:
-there IS a significant increase in excess mortality...due to COVID infection
-there IS NOT a temporal association between vaccines & excess mortality. In fact, quite the opposite: states with the highest vaccination rates had the lowest mortality #VaccinesWork
11/
-there IS a significant increase in excess mortality...due to COVID infection
-there IS NOT a temporal association between vaccines & excess mortality. In fact, quite the opposite: states with the highest vaccination rates had the lowest mortality #VaccinesWork
11/
• • •
Missing some Tweet in this thread? You can try to
force a refresh

































{kind=link}