1/Even attendings have to use google sometimes! Never be afraid to do whatever it takes to get the right diagnosis
A🧵about an interesting spine case that I gasped, “What the…” when I opened it #medtwitter #radres #FOAMed #FOAMrad #neurorad #Meded #backpain #spine #Neurosurgery
A🧵about an interesting spine case that I gasped, “What the…” when I opened it #medtwitter #radres #FOAMed #FOAMrad #neurorad #Meded #backpain #spine #Neurosurgery

2/Older pt w/lower extremity numbness. MRI showed intradural, extra-axial rounded lesions in the lower thoracic region that avidly enhanced on post-contrast imaging—like gang busters enhancement

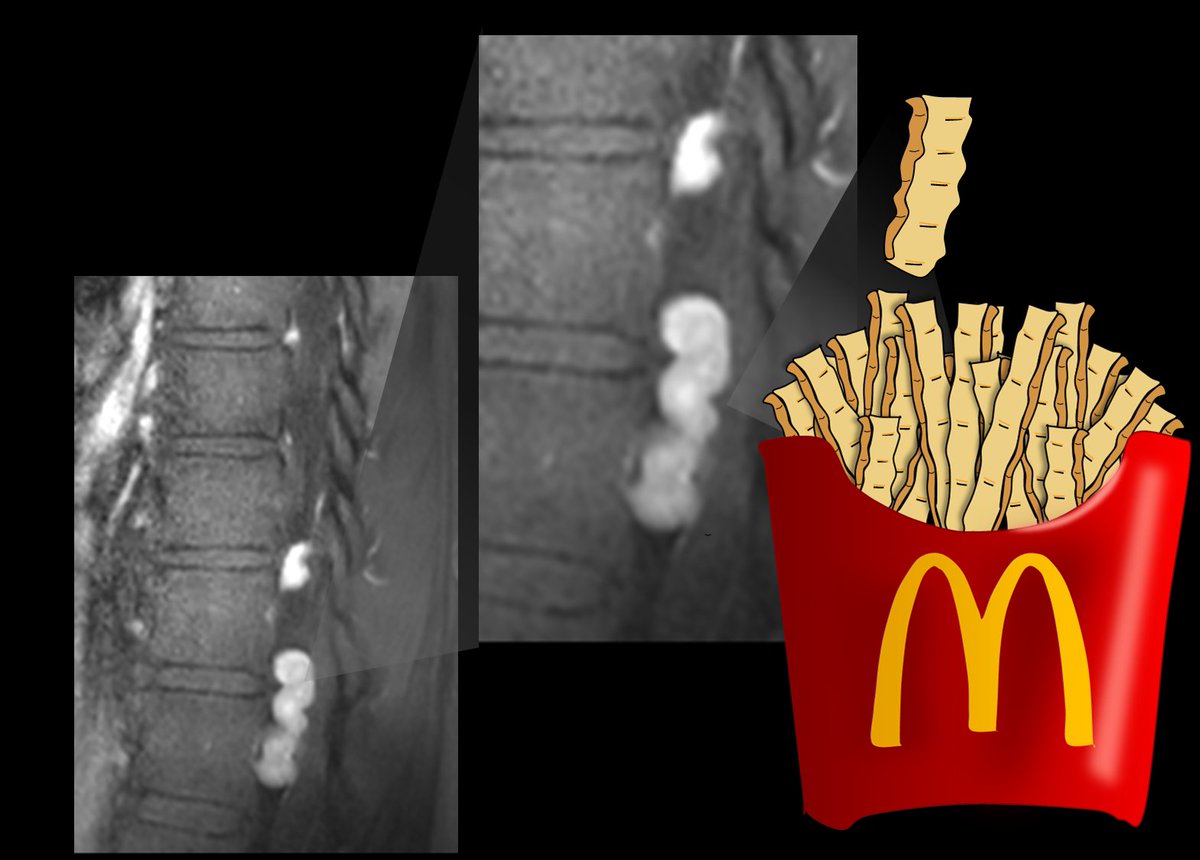
3/On the T2 weighted images, the lesions showed a very distinct donut-like appearance, with a very dark, almost black rim and a bright center.

4/On contrast imaging, the donuts were connected as twisty, tubular structures—my fellow said they looked like crinkle fries! (and yes, I know McDonald’s doesn’t serve crinkle fries as illustrated, but it’s just an illustration—there aren’t fries in the spine either 😉)
5/Tubular sounds like a vessel! And these did empty out into the neural foramina. But the spinal angio was negative for a vascular lesion (not all images shown—normal studies don’t make for good twitter images)
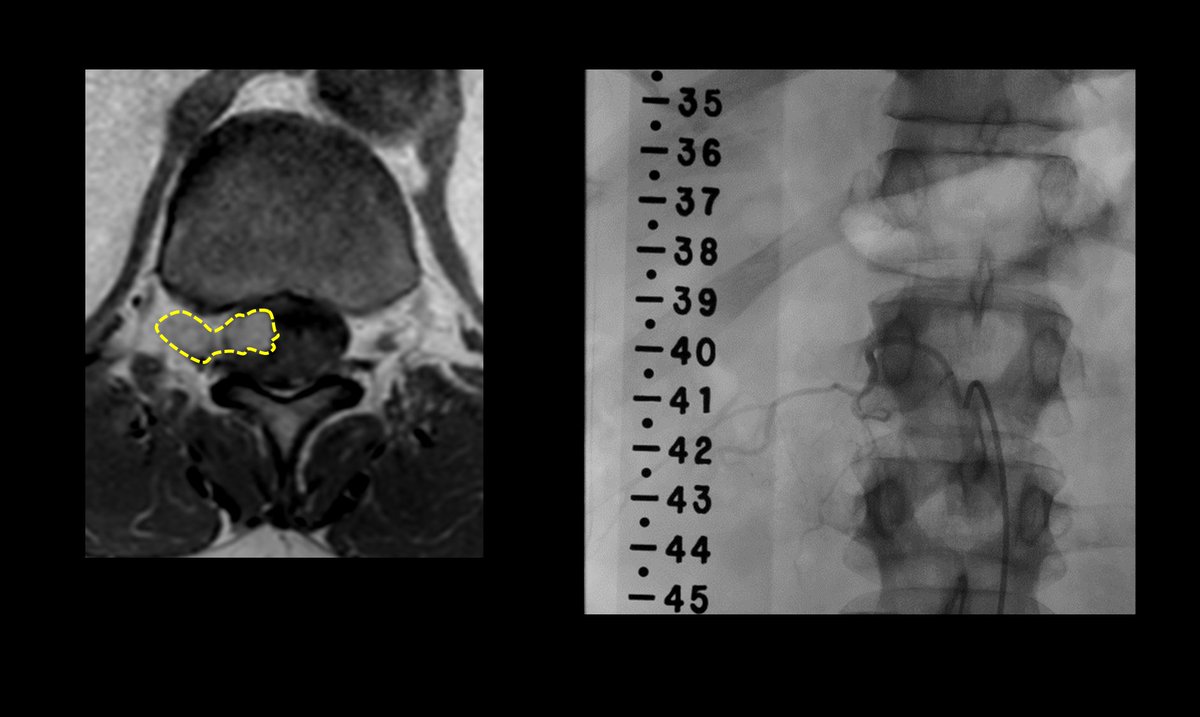
6/These are intradural varices! B/c of slow flow, they may not fill on angiography & lose their flow void centrally—causing a“donut sign.” Etiology is unclear, but likely acquired
So the next time you see donuts & fries in the spine—you can be sure you've got the right diagnosis
So the next time you see donuts & fries in the spine—you can be sure you've got the right diagnosis

• • •
Missing some Tweet in this thread? You can try to
force a refresh