I want to highlight a recent meta-analysis of the sham-controlled renal denervation trials #hypertension
From @maahmed1218 @AndrewFoy82 and others at Penn State.
Free access x 40 days here: sciencedirect.com/science/articl…
Comments >
From @maahmed1218 @AndrewFoy82 and others at Penn State.
Free access x 40 days here: sciencedirect.com/science/articl…
Comments >
They study the 10 sham-controlled trials of RDN. About 1500 patients.
Mean fu (and this is a limitation) = 4 months.
Primary outcomes of the meta-analysis: the *raw mean differences* in 24 hour ambulatory, daytime ambulatory, nighttime, and office SBP and DBP
Mean fu (and this is a limitation) = 4 months.
Primary outcomes of the meta-analysis: the *raw mean differences* in 24 hour ambulatory, daytime ambulatory, nighttime, and office SBP and DBP
Results are clear: RDN does indeed reduce BP.
They found statistically sig reductions in all categories accept nocturnal BP.
Here are the differences in 24 hour ambulatory SBP and office SBP.
They found statistically sig reductions in all categories accept nocturnal BP.
Here are the differences in 24 hour ambulatory SBP and office SBP.


As the authors write, this is not the first meta-analysis of RDN trials, but it is the largest.
Besides the primary finding that RDN does result in modest bp reduction, the authors report some other important findings:
Besides the primary finding that RDN does result in modest bp reduction, the authors report some other important findings:
First is the smaller treatment effect on nighttime BP -- Of course there are potential plausibility explanations:
Mostly, this: "RD aims to reduce BP by reducing a patient's sympathetic output" and of course sympathetic output is less at night.
Mostly, this: "RD aims to reduce BP by reducing a patient's sympathetic output" and of course sympathetic output is less at night.
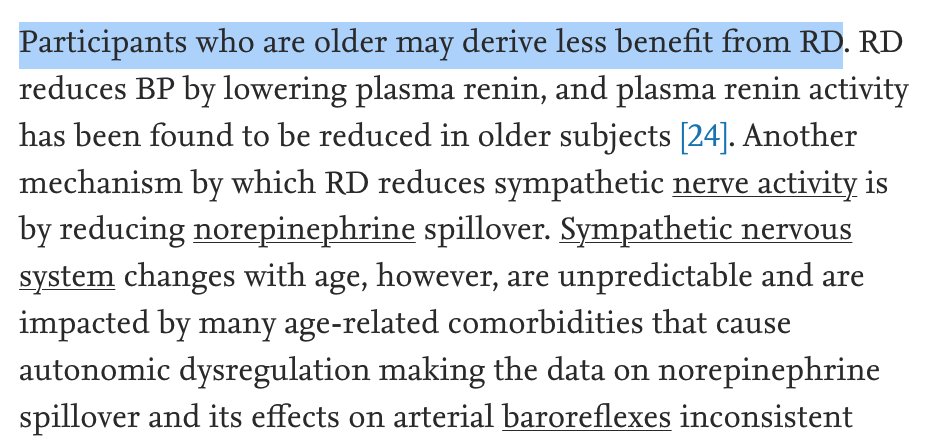
Another finding: there was significant heterogeneity in 3 of the 8 outcomes. A regression analysis suggest that age may play a role in RD effect size.
Like so many things we do there may be less benefit in older patients> see image
Like so many things we do there may be less benefit in older patients> see image
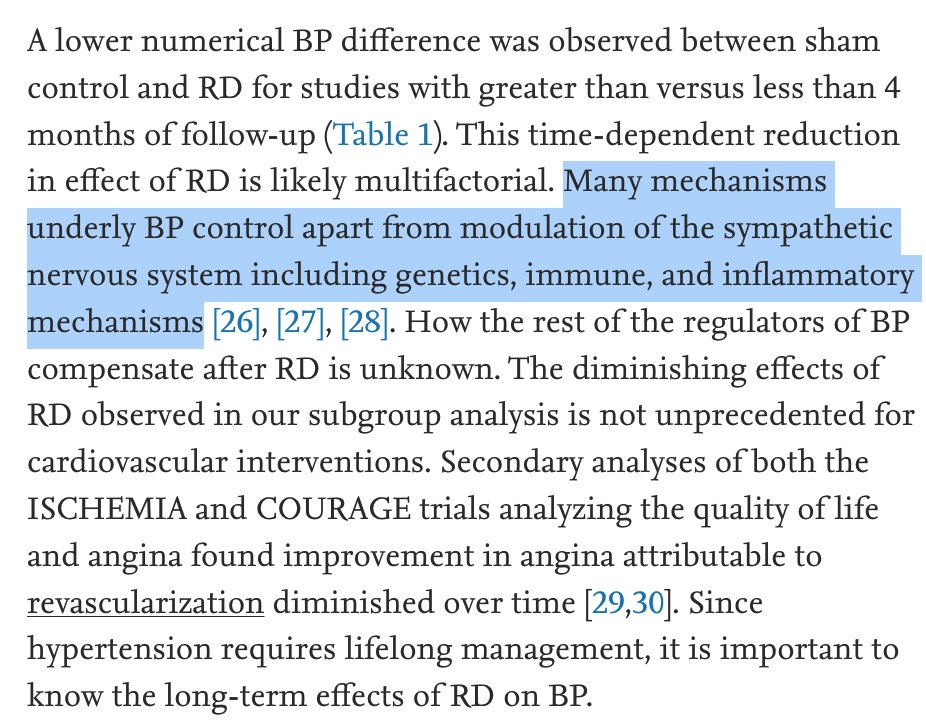
I will finish with the main subgroup finding: length of follow-up.
The differences in BP turned on length of f-u. As the follow-up time got longer, BP reductions were reduced.
This is one of key worry with renal denervation-the durability of effect.
The differences in BP turned on length of f-u. As the follow-up time got longer, BP reductions were reduced.
This is one of key worry with renal denervation-the durability of effect.
The authors discuss the elephant in the room: will RDN lead to better outcomes?
Easy thinking says yes, BP-lowering drug trials have shown that this amount of reduction leads to fewer things like stroke.
But the data from drug trials is much stronger--and longer
Easy thinking says yes, BP-lowering drug trials have shown that this amount of reduction leads to fewer things like stroke.
But the data from drug trials is much stronger--and longer
Proponents of RDN will argue that compliance with tablets is terrible. Hence the benefit from RDN.
The authors however note that compliance can be improved vie system-level initiatives.
See this Kaiser Permanete study >
ahajournals.org/doi/full/10.11…
The authors however note that compliance can be improved vie system-level initiatives.
See this Kaiser Permanete study >
ahajournals.org/doi/full/10.11…
Finally -- I am open-minded about RDN. The authors point out that their meta-analysis include both first and second generation trials.
If you look only at the more modern trials (benefit from iterative improvements) BP reduction is larger.
Could iteration help? Maybe.
If you look only at the more modern trials (benefit from iterative improvements) BP reduction is larger.
Could iteration help? Maybe.
Bottom-line. We need more data. Longer-term data.
Which won't be easy, because to get such, you need to maintain blinding.
B/c one thing is for sure w RDN: without blinding, the data are likely to mislead.
Which won't be easy, because to get such, you need to maintain blinding.
B/c one thing is for sure w RDN: without blinding, the data are likely to mislead.
• • •
Missing some Tweet in this thread? You can try to
force a refresh