1/ Let’s dive into #noninferiority trials for this edition of #StatswithCoreIM
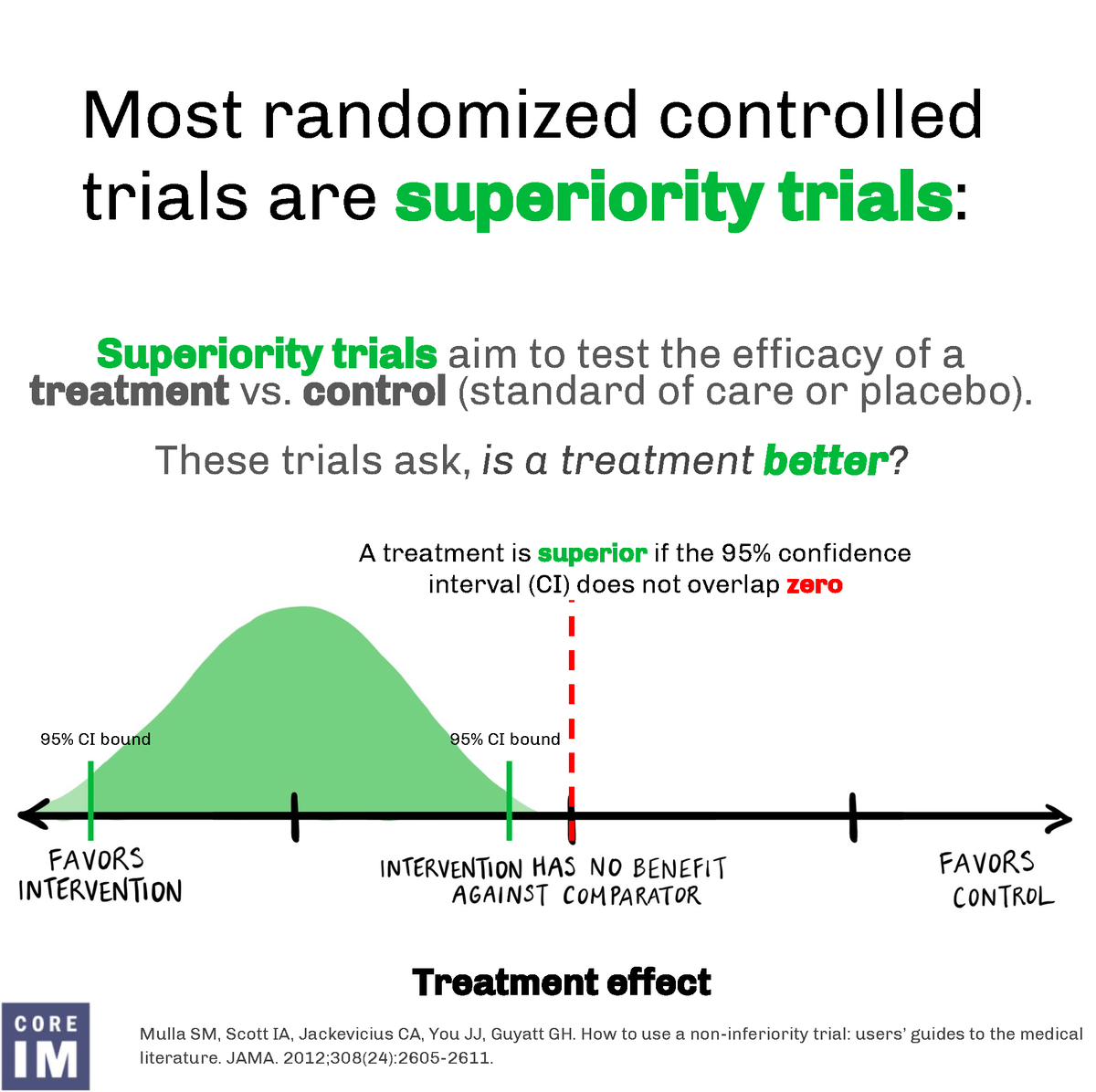
But first, take a look at this figure for what superiority trials aim to assess: What’s better?
But first, take a look at this figure for what superiority trials aim to assess: What’s better?
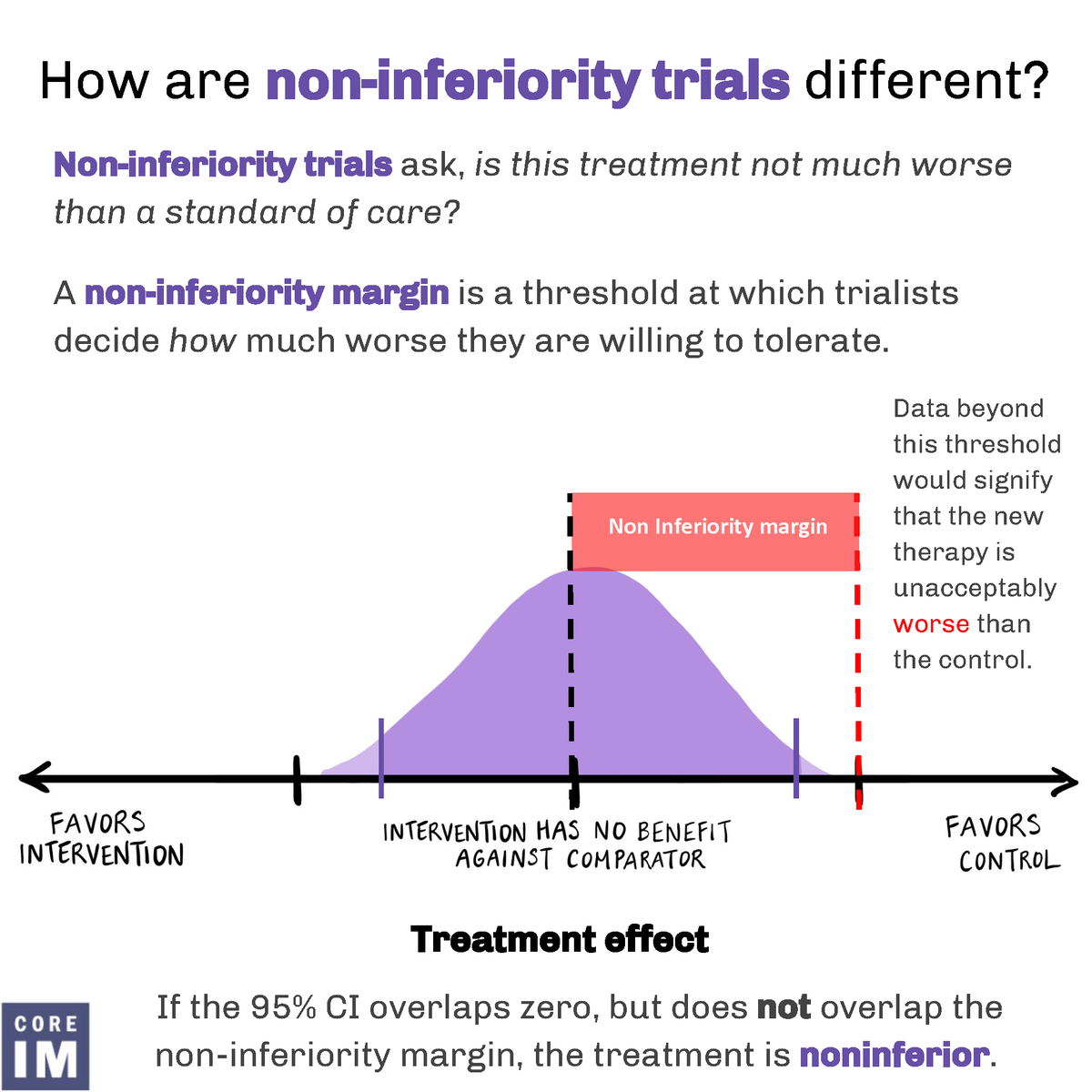
2/ So how are NON-inferiority trials different?
They ask if a treatment is much worse than standard of care.
They ask if a treatment is much worse than standard of care.
3/ Let’s look at the possible outcomes of a non-inferiority trial.
✔️Superior and non-inferior
✔️Non-inferior
✔️Not non-inferior
✔️Inferior and not non-inferior
✔️Inferior and non-inferior
✔️Superior and non-inferior
✔️Non-inferior
✔️Not non-inferior
✔️Inferior and not non-inferior
✔️Inferior and non-inferior

4/ To close, why do a non-inferiority trial?
✅There is an accepted std of care, so placebo controlled may be unethical
✅If a new treatment is unlikely to outperform std of care
✅If a new treatment is similar to existing treatments, but may have un-tested benefits
✅There is an accepted std of care, so placebo controlled may be unethical
✅If a new treatment is unlikely to outperform std of care
✅If a new treatment is similar to existing treatments, but may have un-tested benefits

5/ Thanks to our awesome team! Shoutout to the author of this byte Dr. Robert Wharton and graphics by @ivannatang
• • •
Missing some Tweet in this thread? You can try to
force a refresh