
1/Do radiologists sound like they are speaking a different language when they talk about MRI? T1 shortening what?T2 prolongation who?
Here’s a translation w/a #tweetorial introduction to MRI
#medtwitter #FOAMed #FOAMrad #medstudent #neurorad #radres @MedTweetorials #neurosurgery
Here’s a translation w/a #tweetorial introduction to MRI
#medtwitter #FOAMed #FOAMrad #medstudent #neurorad #radres @MedTweetorials #neurosurgery

2/When it comes to bread and butter neuroimaging—MRI is definitely the butter. Butter makes everything taste better and packs a lot of calories. MRI can add so much information to a case

3/In fact, if CT is a looking glass into the brain—MRI is a microscope. It can tell us so much more about the brain and pathology that affects the brain. So let’s talk about the basic sequences that make up an MRI and what they can show us.

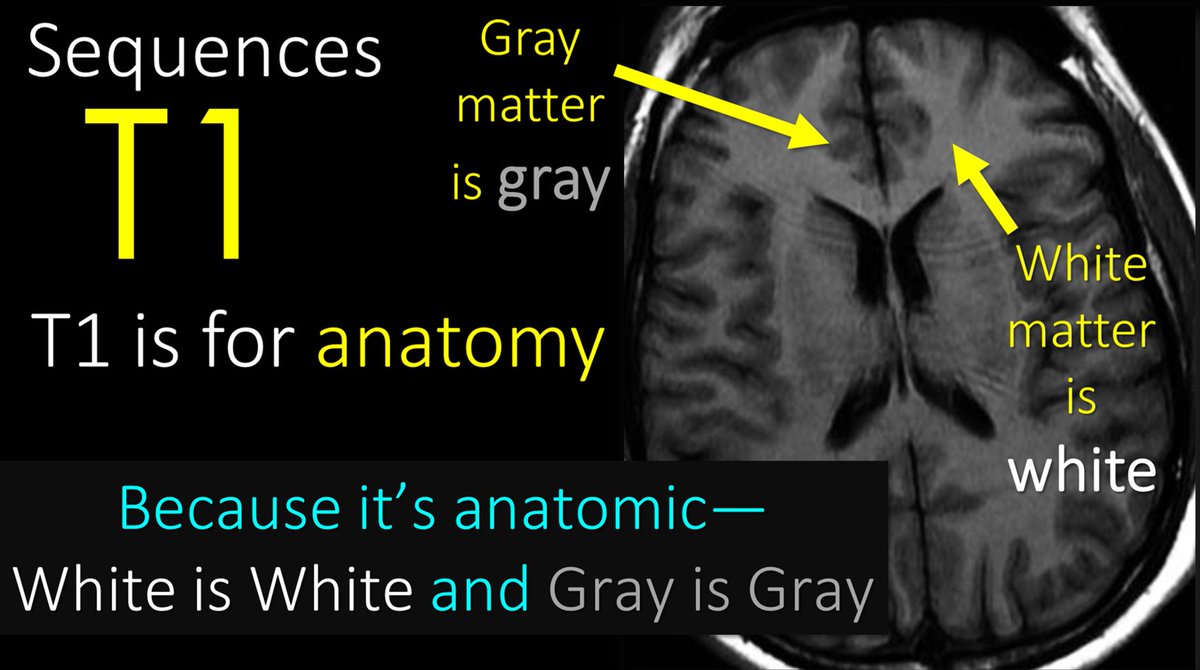
4/Let’s start w/T1—it is #1 after all! T1 is for anatomy. Since it’s anatomic, brain structures will reflect the same color as real life. So gray matter is gray on T1 & white matter is white on T1. So if you see an image where gray is gray & white is white—you know it’s a T1.
5/T1 is also for contrast. Contrast material helps us to see masses. Contrast can’t get into normal brain & spine bc of the blood brain barrier—but masses don’t have a blood brain barrier, so when you give contrast, masses will take it up & light up, making them easier to see.

6/So to review, T1 is for anatomy and contrast. I remember this bc anatomy is the number 1 thing a radiologist needs to know and a mass is the number 1 thing a radiologist doesn’t want to miss.

7/Now to T2! T2 sequences are water sensitive sequences. What is pathologic water in the brain? Edema! My attending once said, “Everything bad in this world is trying to turn you back into what you came from—water. So T2 shows you edema—but this edema can be from many things.

8/To review—T1 is for anatomy and contrast, T2 (and FLAIR, which is a type of T2) is for water—which is bright on T2. I remember this bc H20 has a 2 in it—T2 is for H20.

9/Next to diffusion or DWI. Diffusion is primarily to detect stroke. Acute strokes are bright on diffusion. But just as all that glitters is not gold, not all that is bright on DWI is an acute stroke.

10/This is bc all diffusion does is detect how difficult it is for water to move. Anything that makes the space around water crowded and difficult to move will be bright on diffusion imaging

11/So classically, it from a stroke. When cells run out of ATP, the Na/K pump stops working & immediately water rushes in from osmotic pressure & the cells swell. These swollen cells fill the interstitium & restrict the movement of water. This is why strokes are bright on DWI!

12/But other things can make it crowded and difficult for water to move. For example, tightly packed cells in aggressive tumors will also fill the spaces & make it difficult for water to move—it is trapped between the tumor cells! So highly cellular tumors are often bright on DWI

13/Here is an example. Here is a mass that is as bright as stroke on diffusion bc of its densely packed cells. On contrast images, we see it avidly enhance, as we would expect for a mass. On CT, the tumor is very dense bc of the densely packed cells.

14/Hematomas are also bright on DWI. In normal blood, water flows happy & free—but once the clotting cascade starts & fibrin & thrombin & whatever stuff I don’t remember as a radiologist clumps everything together, things get tight—water is trapped in the clot interstices!

15/Here is an example. The hemorrhage is bright on CT bc it is clotted, and thus more dense than the brain and CSF, which are closer in density to water. For this same reason, the hemorrhage is bright on diffusion—bc the dense clot traps the water.

16/Pus is also bright on diffusion. As a radiologist I don’t often see pus, but as a mom, I sure do. It is thick and gooey and you can just imagine how difficult it is for water to travel through that gelantinous blob of pus.

17/Here’s an example. There is a ring enhancing lesion w/a lot of edema on T2. Centrally, there is restricted diffusion, meaning that there is something gooey or thick or dense centrally. Bc this central stuff doesn’t enhance, we know it’s not a mass. This is pus in an abscess!

18/So to review--while not everything that is bright on diffusion is a stroke, the most important use is for strokes. I remember this bc it's called DWI--which I joking say stands for Diagnose With Infarct!

19/Last but not least is gradient imaging. Gradient imaging is sensitive to metals. And what’s the most important metal in body? Iron—bc iron is in blood. So gradient is our blood sensitive sequence

20/Blood is black on gradient. I remember this bc gradient is for metal—and when I think of metal, I think of blacksmiths forging metal products. So BLACKsmith=metal is BLACK on gradient.

21/But other metals will be black too. Notably, calcium, which is in our bones and in many other lesions. So remember, just all that glitters is not gold, not all that is black on gradient is blood—other metals are black too

22/So now you know the basic MRI sequences and what they are used for. So hopefully now, the radiologist won’t sound like they are speaking a different language when they talk to you—they will just be nerdy and socially awkward when they do!

• • •
Missing some Tweet in this thread? You can try to
force a refresh





















