
12 Principles for rounding and case presentations for medical students,
residents, and attendings who are forever residents at heart
#medtwitter
#neurotwitter
residents, and attendings who are forever residents at heart
#medtwitter
#neurotwitter

Whether you are presenting to the attending or calling in a consult,
it is your responsibility to convince
it is your responsibility to convince

Where is this going?
Are you lost?
I am!
Are you lost?
I am!
Isn't this better?
The Chief Complaint guides the rest of the presentation
The Chief Complaint guides the rest of the presentation
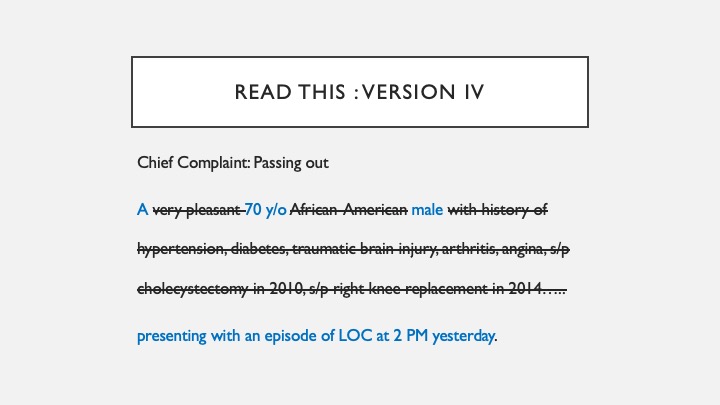
Always start with the chief complaint OR reason for consultation.
This helps anchor the listener to a symptom/sign/scenario
and they can start developing differential for the case.
This helps anchor the listener to a symptom/sign/scenario
and they can start developing differential for the case.
Don’t need to know if he is pleasant or not; don’t need to know race in most cases.
Might matter if the patient does not speak English. So you can say Indian with limited English communication coz now that has an impact on whether you are going to get reliable history.
Might matter if the patient does not speak English. So you can say Indian with limited English communication coz now that has an impact on whether you are going to get reliable history.
This is even better!
In most cases, "Past Medical History" should be limited to "Past Medical History"
In most cases, "Past Medical History" should be limited to "Past Medical History"
Your listener will thank you!
There are likely some exceptions in every specialty. For ex. in Neurology:
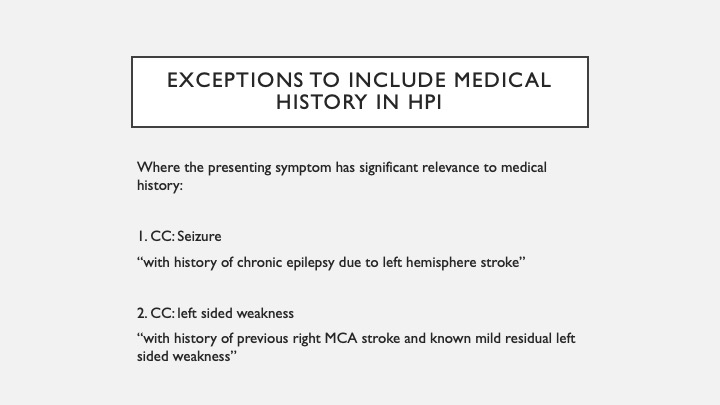
h/t @Dr_Oubre
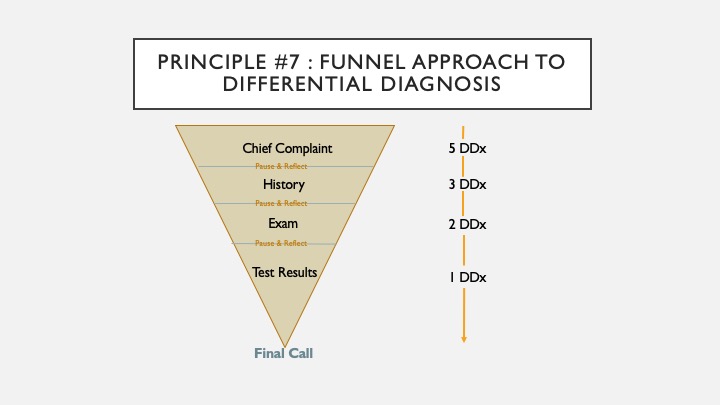
@Dr_Oubre As you proceed to listen and present each aspect of the presentation, the number of differential diagnoses should narrow down.
@Dr_Oubre Most services will have a patient cap for residents. Collecting relevant data before rounds can be easily done and save a huge amount of time during rounds.
You can argue why to note the data when it is easily available in the EMR.
Try both. The suggested process is better
You can argue why to note the data when it is easily available in the EMR.
Try both. The suggested process is better
@Dr_Oubre Medications are beneficial toxins but toxins nonetheless.
The commonest consult in neurology is Altered mental status. Very common to have medications as the offender.
The commonest consult in neurology is Altered mental status. Very common to have medications as the offender.
@Dr_Oubre Summary:
1. Presenter's job to convince listener
2. Start with chief complaint
3. Filter out the irrelevant (PMH)
4. Tell it chronologically
5. Keep positives and negatives together
6. Why is the patient presenting now?
1. Presenter's job to convince listener
2. Start with chief complaint
3. Filter out the irrelevant (PMH)
4. Tell it chronologically
5. Keep positives and negatives together
6. Why is the patient presenting now?
@Dr_Oubre Summary:
7. Funnel approach to differential diagnoses
8. Keep relevant data handy
9. Compare and contrast imaging
10. It's all about the medications
11. Cheat but confirm
12. Supplementary information is everything
Anything you would like to add?
7. Funnel approach to differential diagnoses
8. Keep relevant data handy
9. Compare and contrast imaging
10. It's all about the medications
11. Cheat but confirm
12. Supplementary information is everything
Anything you would like to add?
@Dr_Oubre This account exists to teach and share essential physician-specific knowledge that is untaught.
If you enjoyed this thread:
1. Follow me @rohitmarawar for more of these
2. RT the tweet below to share this thread with your audience
If you enjoyed this thread:
1. Follow me @rohitmarawar for more of these
2. RT the tweet below to share this thread with your audience
https://twitter.com/rohitmarawar/status/1541445768128724992
• • •
Missing some Tweet in this thread? You can try to
force a refresh



