1/Is remembering cerebellar anatomy making you dizzy? Need help telling your flocculus from your nodule?
Here’s some help w/a #anatomy #tweetorial on the 9 lobules of the vermis!#medtwitter #FOAMed #FOAMrad #medstudent #neurorad #radres @medtweetorials #neurosurgery @StefanTigges
Here’s some help w/a #anatomy #tweetorial on the 9 lobules of the vermis!#medtwitter #FOAMed #FOAMrad #medstudent #neurorad #radres @medtweetorials #neurosurgery @StefanTigges

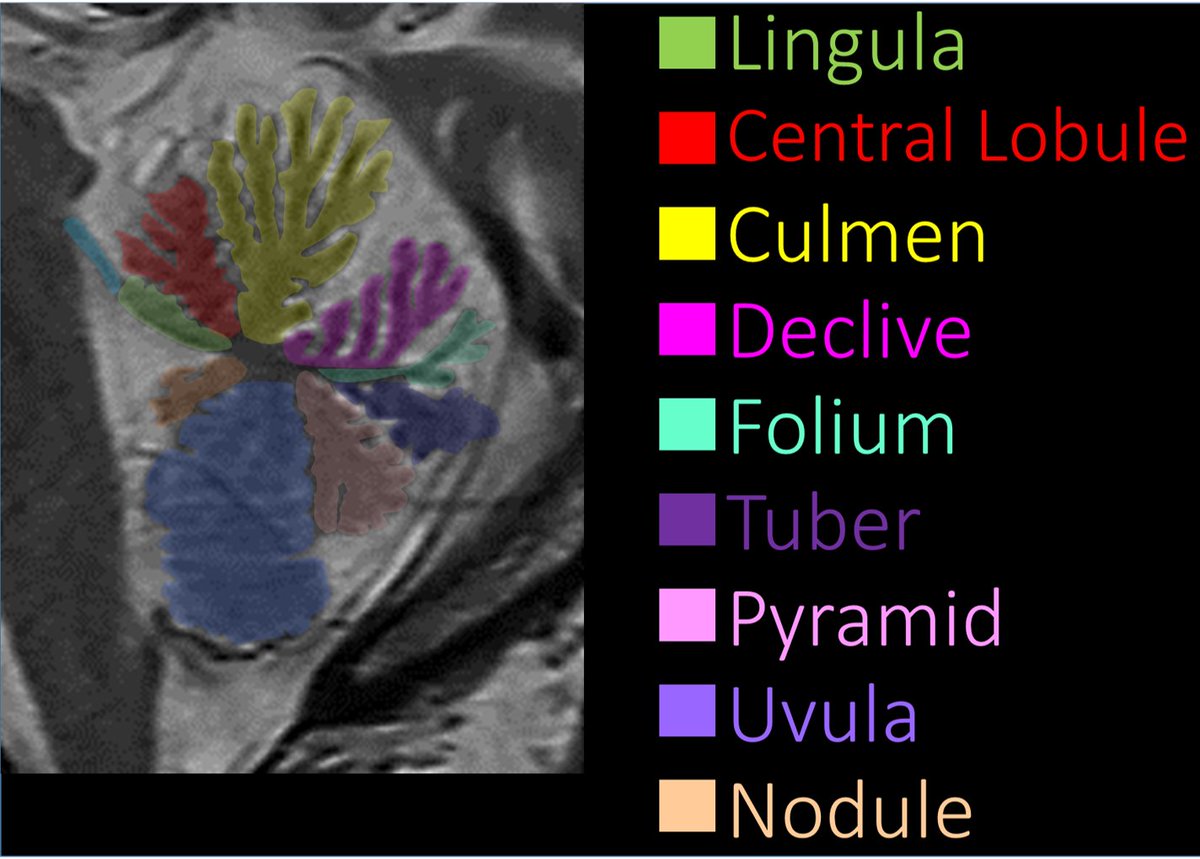
2/Coming from anterior, the first lobule is the lingula. It sticks out from the front of the vermis & is connected to the superior cerebellar peduncle. I remember this bc it has a very appropriate name—lingula—it looks like a tongue sticking out of the vermis to lick the SCP.

3/Moving clockwise, next is the central lobule. I remember this bc it is positioned exactly how a central lobule should be positioned, in the driver’s seat—where the front seat driver position would be if the vermis was a car—up front, looking out the windshield over the lingula

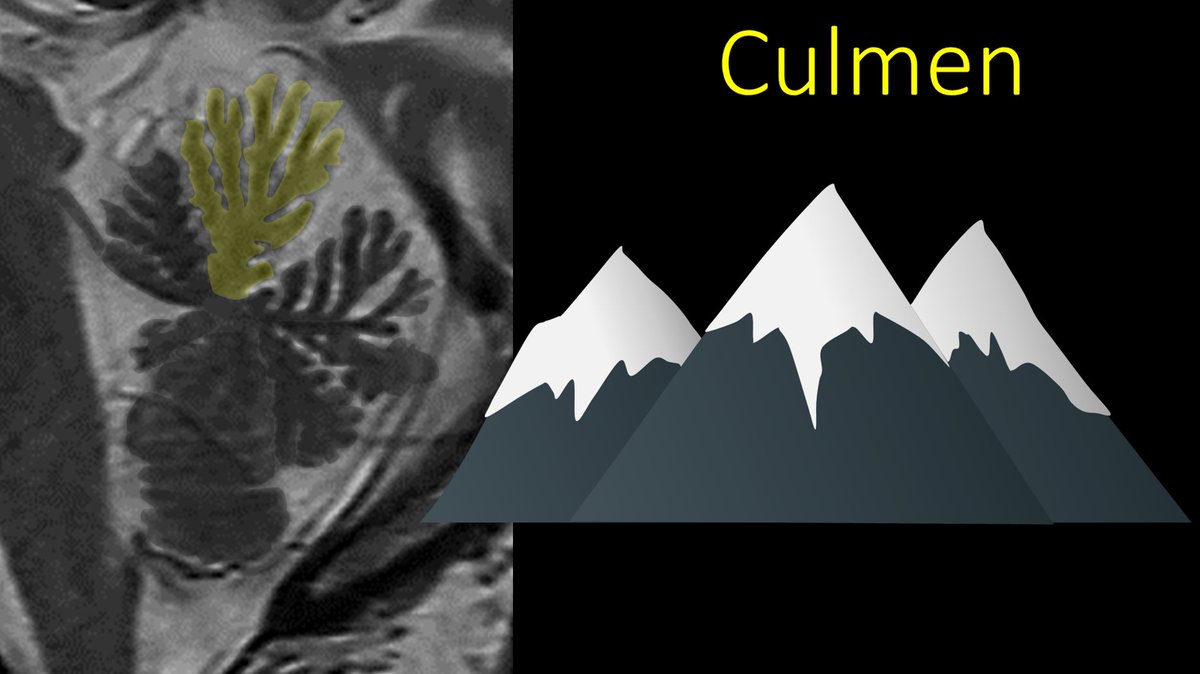
4/Next lobule over is the culmen. I remember this bc culmen sounds like culminate—which means to reach the highest altitude—and that’s what the culmen is—it is the highest point—the mountain peak of the vermis.
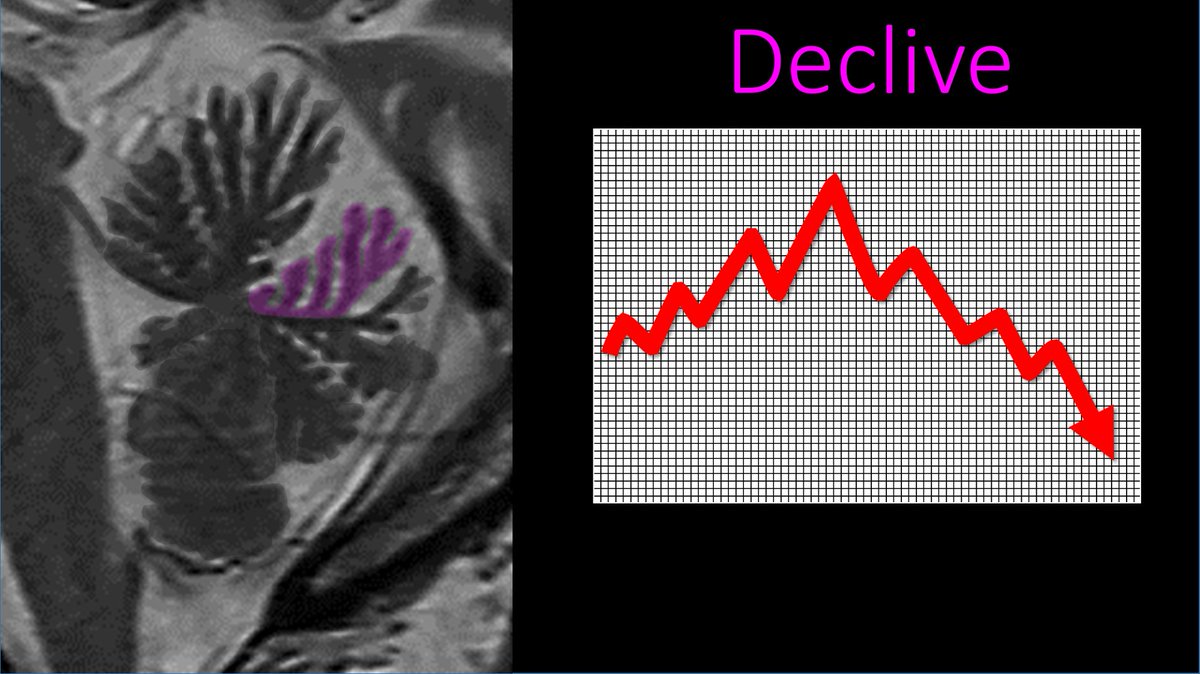
5/Next is the declive. This is easy to remember bc after reaching the peak of the culmen, what happens next? We have to go down or decline = declive. The declive is the lobule that starts to go down after the culmen—not unlike our current stock market 😬
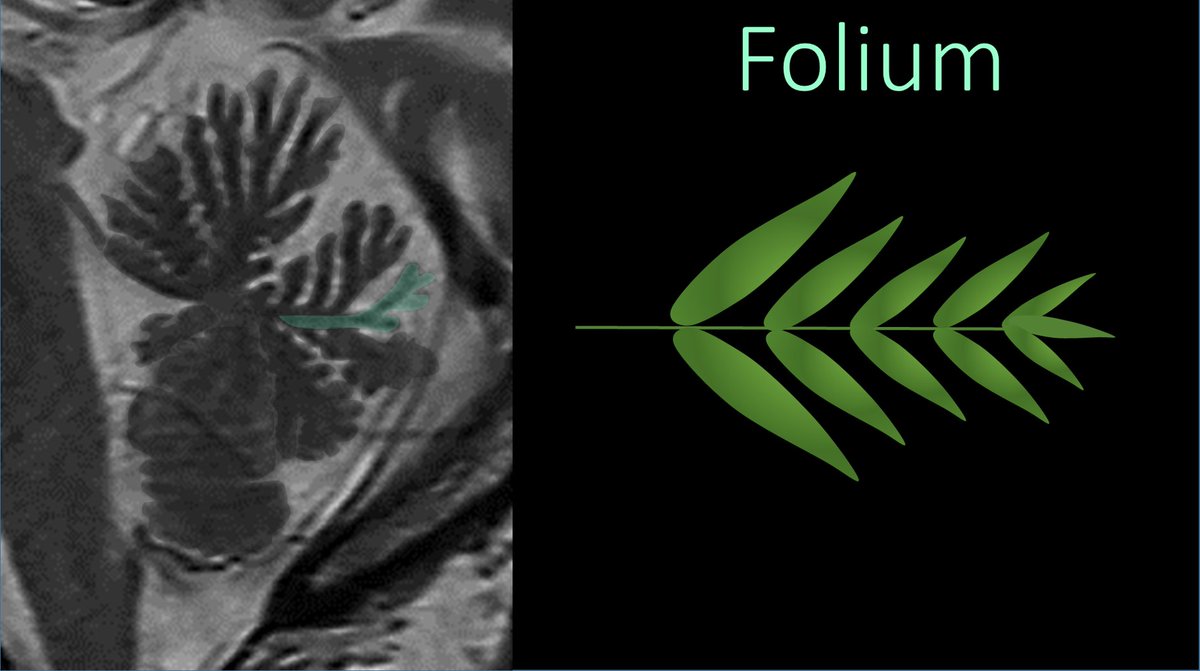
6/After declive is the folium. I remember this bc it looks like a thin fern branch, or “foliage,”with a thin stem and just a thin layer of leaves
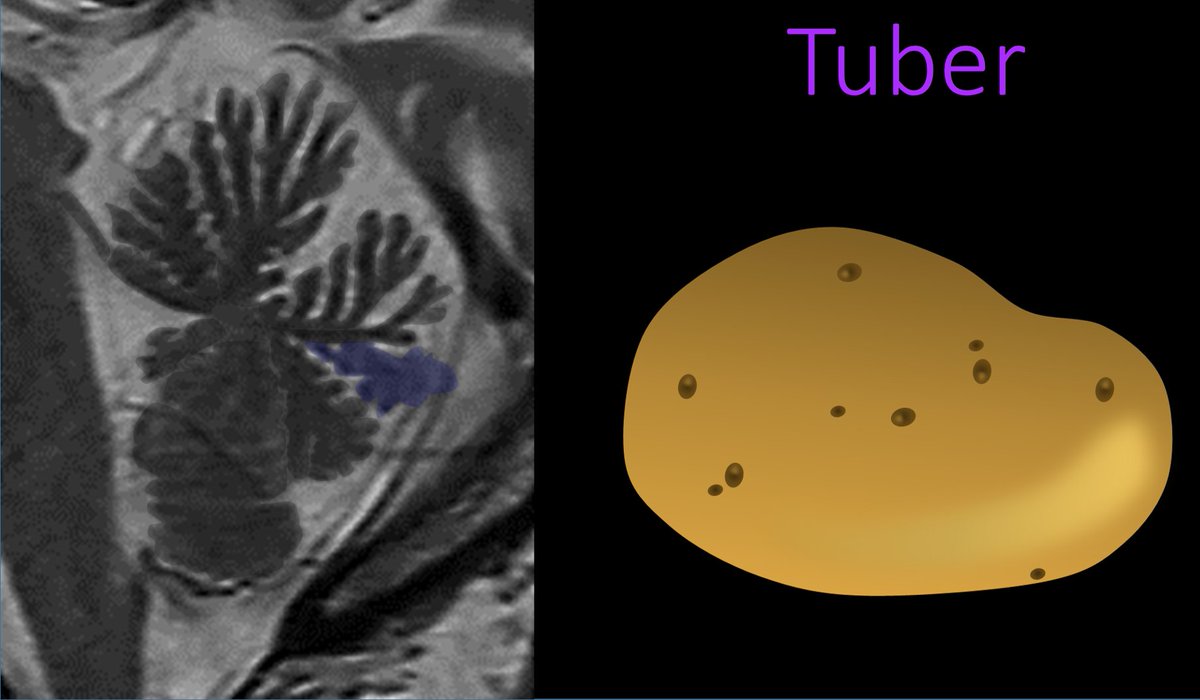
7/The tuber follows the folium. It is similar to the folium, except instead of being thin like a fern branch, it is much chunkier, with thicker nodules on it. Hence its name is easy to remember—tuber means potato, and this lobule has a fatter, rounder contour like a potato.
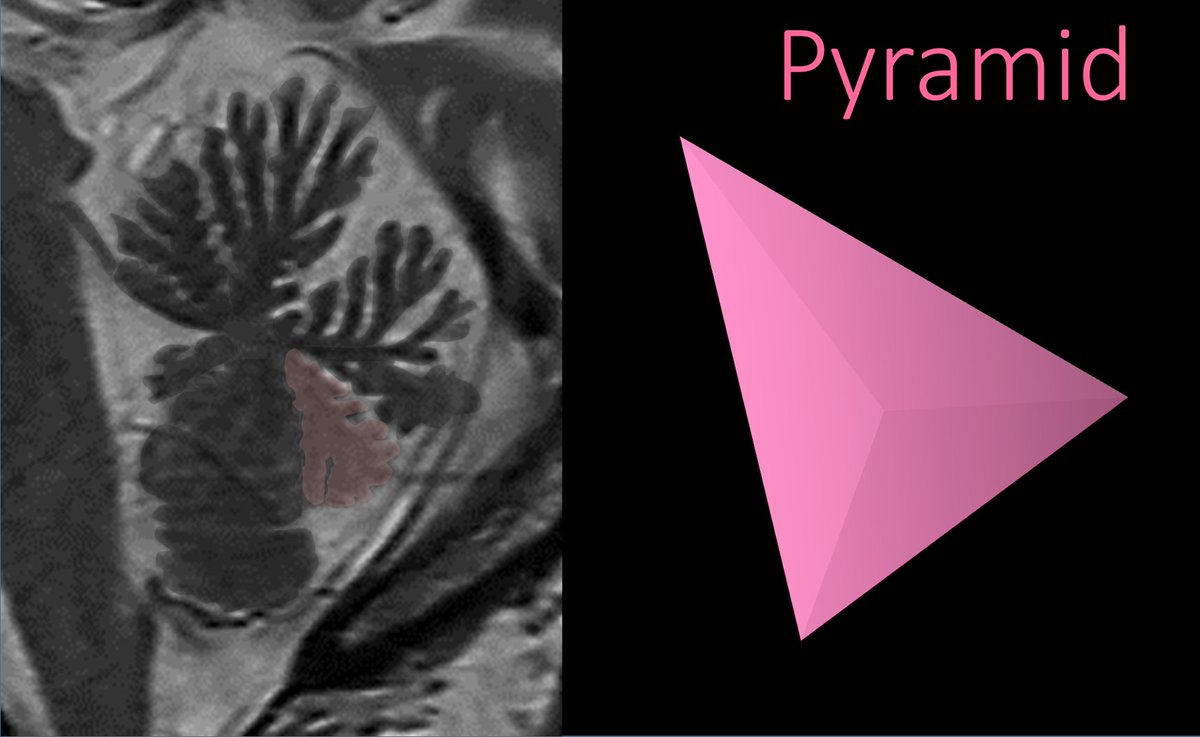
8/As we continue around, next is the pyramid. This one is easy to remember—it is triangular like a pyramid, and hence its name
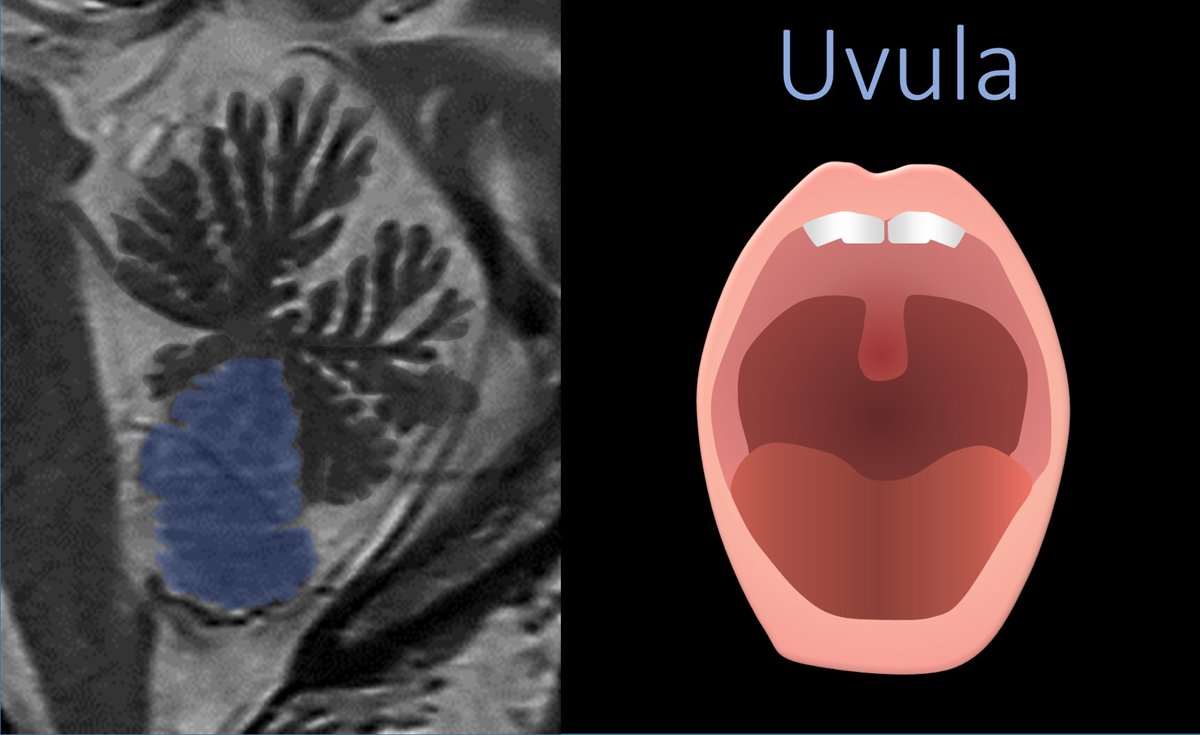
9/Hanging down from the bottom of the vermis is the uvula. It is easy to remember how they named this one. It hangs down from the vermis just like your uvula hangs down from the roof of your mouth.
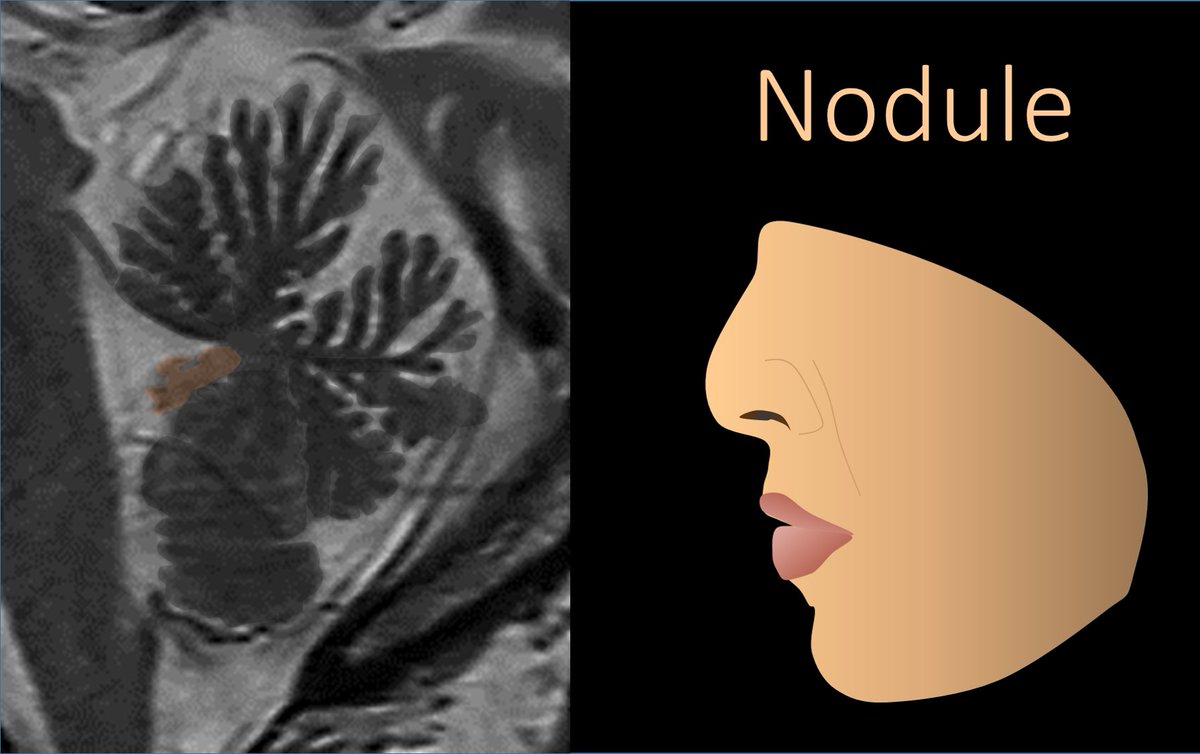
10/Last is the nodule. I remember this bc nodule sounds like nose--and it even looks like a nose—pointing out from the middle of the vermis the way the nose points out of the middle of your face.
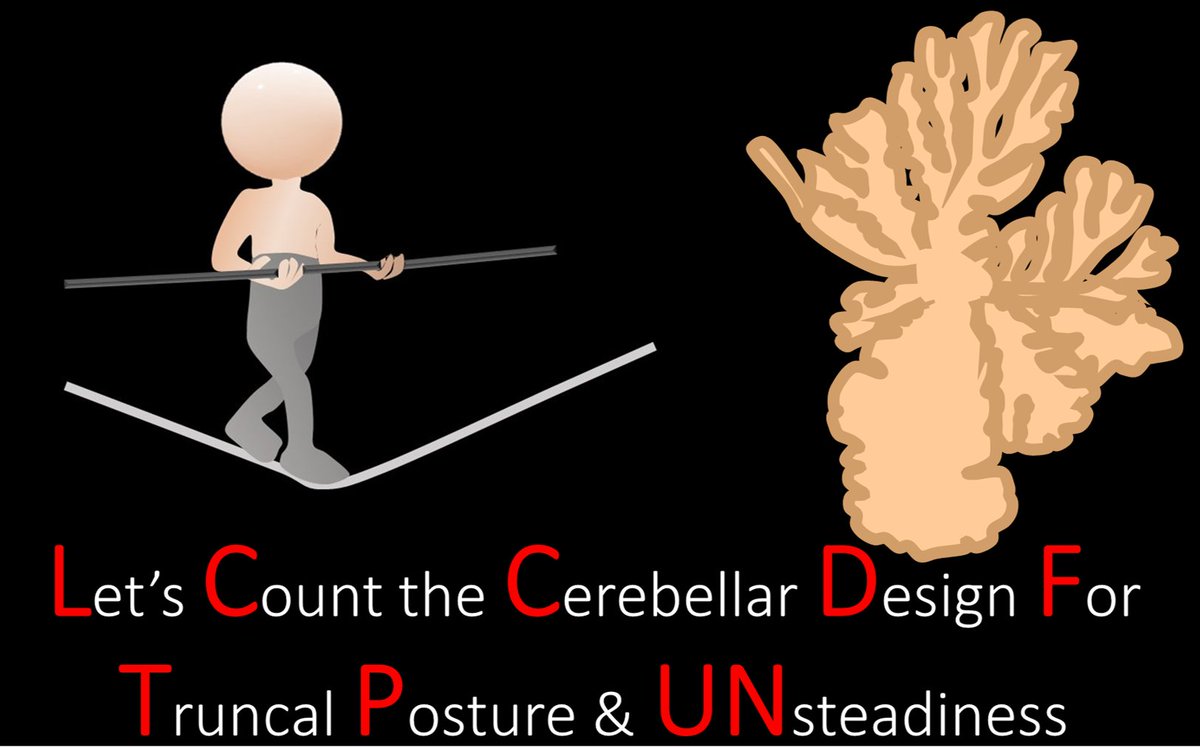
11/”Ok,” you might say, “Now I can remember the names, but how can I remember the order?” I’ve got your back. The vermis is important for truncal balance, so my mnemonic is “Let’s Count the Cerebellar Design for Truncal Posture and Unsteadiness.”
12/So now you know how to remember all the lobules of the vermis and have a mneumonic to remember their order. May your knowledge continue to culminate and never declive!
• • •
Missing some Tweet in this thread? You can try to
force a refresh