During med residency in late 1990s, I noticed that patients w/ hypermobile joints ("double jointed") frequently had episodes of unexplained tachycardia, headache/lightheadedness.
I suspected Marfan's but never found the classic signs for it (i.e., tall stature, high arched palate, or "thumb sign" [see images below from nature.com/articles/52018… ]).
Plus, for whatever reason, many of these patients were women.
Plus, for whatever reason, many of these patients were women.

So I chalked this to some unknown connective tissue disorder which may/may not have some relationship with these symptoms.
Years later, I found out that these patients likely had Ehler-Danlos syndrome #EDS. (Yes, I should have known, but my Harrison's textbook was no UptoDate).
Years later, I found out that these patients likely had Ehler-Danlos syndrome #EDS. (Yes, I should have known, but my Harrison's textbook was no UptoDate).
Even more recently, I found out that many EDS patients suffer from #dysautonomia (specifically, #POTS).
In a recent retrospective analyses of 98 EDS patients, nearly 80% had dysautonomia presenting w/ palpitations, dizziness and syncope.
In a recent retrospective analyses of 98 EDS patients, nearly 80% had dysautonomia presenting w/ palpitations, dizziness and syncope.


So what is the pathophysiological link between #EDS and #POTS?
Apparently, the answer's still unclear but few hypotheses exist:
Apparently, the answer's still unclear but few hypotheses exist:
1.) Lower extremity have highly distensible vasculature that lead to low PVR (arteries/arterioles) and pooling of blood (veins) upon standing. The reduced venous return does not necessarily lead to hypotension, but sympathetics NS compensation leads to tachycardia/palpitations.
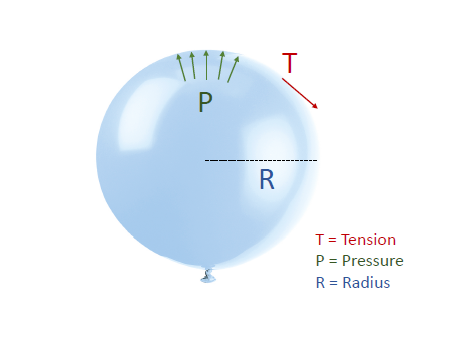
2.) Baroreceptors in carotid/aortic bodies are located in the tunica adventitia of vessel, amidst loose connective. The highly compliant connective tissue do not generate high wall stresses so baroreceptors are not activated even during systole.
Baroreceptors thus chronically sense low pressure and hence activate the SNS.
This explains why EDS patients were found (via autonomic tests) to have "resting sympathetic overactivity but decreased sympathetic reactivity to stimuli".
Of note, Parasympathetic NS remained intact.
This explains why EDS patients were found (via autonomic tests) to have "resting sympathetic overactivity but decreased sympathetic reactivity to stimuli".
Of note, Parasympathetic NS remained intact.

3.) Use of vasoactive medications (like opiates, trazodone, antihypertensives, TCA, etc) in this population may also contribute to dysautonomia - but I would probably guess it plays a minor role.
Figure from dx.doi.org/10.1016/j.sema…
Figure from dx.doi.org/10.1016/j.sema…
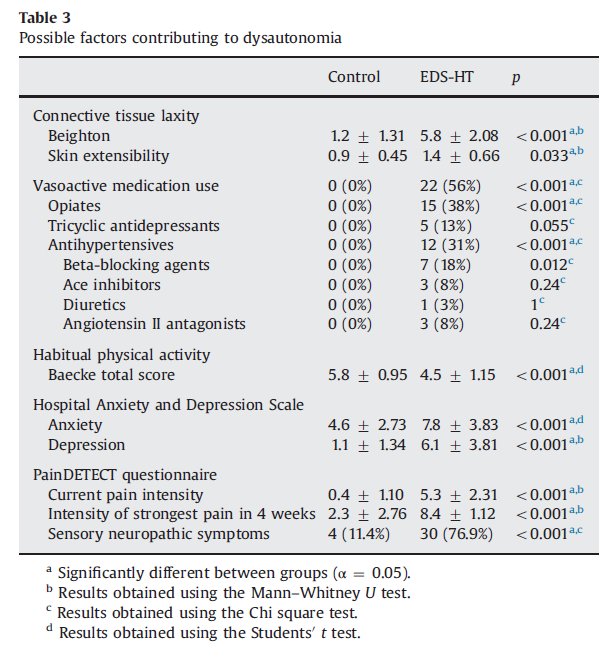
From this same publication, it was evident that level of distensibility was quite important:
".... we found that parameters reflecting collagen laxity, such as skin extensibility and the Beighton score, were related to parameters of vasodilatation .. and to increased HR...
".... we found that parameters reflecting collagen laxity, such as skin extensibility and the Beighton score, were related to parameters of vasodilatation .. and to increased HR...
... Moreover, in the linear regression analysis, skin extensibility was identified as the most important predictor for the severity of sympathetic dysfunction, stronger than vasoactive medication use."
These autonomic NS symptoms are not trivial and can be debilitating.
In 2019, Ms. Nicola Blackwood - a prominent member of the UK parliament then - passed out during a congressional session. She has made her EDS and POTS diagnosis quite public.
In 2019, Ms. Nicola Blackwood - a prominent member of the UK parliament then - passed out during a congressional session. She has made her EDS and POTS diagnosis quite public.
And EDS is increasingly being associated with #MECFS and #LongCOVID.
Notably, it is primarily the hypermobile type of EDS (hEDS) that is showing this link. So some mechanical feature of connective tissue is somehow central to the pathophysiology.
Notably, it is primarily the hypermobile type of EDS (hEDS) that is showing this link. So some mechanical feature of connective tissue is somehow central to the pathophysiology.
https://twitter.com/Be_Kinderr/status/1420153840666562563
Ultimately, autonomic dysfunction in hEDS is very common and greatly underappreciated. Surprisingly little is known about the underlying mechanism. There is a lot more to connective tissue physiology than we know. Keep an eye on this space.
End/
End/
• • •
Missing some Tweet in this thread? You can try to
force a refresh