
ICU POCUS snippets: Much has been said about how useful lung POCUS is for procedural guidance. First of all, it accurately reveals large effusions when the radiology report characterizes them as “small”. This is from a recent case of a pt intubated w community-acquired pneumonia 

and what proved to be bilateral parapneumonic effusions:
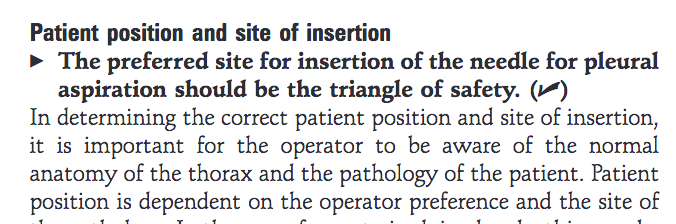
Secondly, while the dogma (which, btw, I don’t recommend completely ignoring!) in thoracentesis is to insert the needle at the “triangle of safety”, bordered by the anterior border of the latissimus dorsi, the lateral border of the pectoralis major, the horizontal line at the...
... level of the nipple, and an apex below the axilla, the lung POCUS usually gives a clear view of alternative “landing area(s)” and allows placement at a much lower level than the nipple line. This is from the 2010 British Thoracic Society Guidelines (thorax.bmj.com/content/65/Sup…)

that recommend needle insertion inside the triangle:
And this is where the needle - and pigtail - were inserted w POCUS assistance. Side note: I do not usually ask the staff to sit the mechanically ventilated patients up and keep them "steady"; it's very hard for them, especially in obese patients...

CXR (1.8 liters later):

Finally, if you want to be extra extra cautious, it’s better to: i) scan for intercostal vessels with 2D and color Doppler in the spot where you plan to insert the needle, and ii) aim the needle towards the bed, ...
... not parallel to it or anteriorly, since, in general, a splenic biopsy is less risky than a cardiac one!
This is a useful reference: Better with ultrasound: Pleural procedures in critically ill patients. Millington SJ, Koenig S. Chest 2018. 153(1): 224-32. PMID: 28736305
This is a useful reference: Better with ultrasound: Pleural procedures in critically ill patients. Millington SJ, Koenig S. Chest 2018. 153(1): 224-32. PMID: 28736305
Thanks for reading!
#POCUS #POCUSpeeps #FOAMed #FOAMus #FOAMcc #IMPOCUS #MedTwitter #MedEd #EMBound @ACEP_EUS @MetroHealth_EM @MH_EMultrasound @RJonesSonoEM @jaffa_md @katiewiskar @kyliebaker888 @TomJelic @msiuba @siddharth_dugar @thepocusatlas @ICUltrasonica @khaycock2
#POCUS #POCUSpeeps #FOAMed #FOAMus #FOAMcc #IMPOCUS #MedTwitter #MedEd #EMBound @ACEP_EUS @MetroHealth_EM @MH_EMultrasound @RJonesSonoEM @jaffa_md @katiewiskar @kyliebaker888 @TomJelic @msiuba @siddharth_dugar @thepocusatlas @ICUltrasonica @khaycock2
@NickjohnsonMD @EmergenxyPhysic @pocusmeded @POCUSClub @thepocusatlas @TaotePOCUS @pocusfoamed @interconsulta @cianmcdermott @nickmmark @cjosephy @pdsalinas @KalagaraHari @UAlberta_Sono @EMUGs_ @UAlberta_ICU @UAB_Sono @EMUGs_ @MedCriticaMex @critconcepts
• • •
Missing some Tweet in this thread? You can try to
force a refresh






