1) Pregnancy is a significant sociocultural event in human society.
It marks the sacred connection between one generation and its offspring.
This is what most people think.
Let me tell you why its not --> through the lens of evolutionary medicine.
It marks the sacred connection between one generation and its offspring.
This is what most people think.
Let me tell you why its not --> through the lens of evolutionary medicine.

2) Pregnancy is actually a vicious battle between two partially related genetic entities --> the mother and its fetus.
Neither side shows mercy or takes prisoners.
We will focus on the battle for fuel at the fetomaternal interface in this Tweetorial.
Neither side shows mercy or takes prisoners.
We will focus on the battle for fuel at the fetomaternal interface in this Tweetorial.
3) First of all --> the physiology.
The pregnant female usually experiences reset homeostasis --> with fasting blood sugar (FBS) gradually falling till the week 12 --> then it stabilizes till term.
But PPBS shows sharper, more sustained rise, along with rising insulin levels!
The pregnant female usually experiences reset homeostasis --> with fasting blood sugar (FBS) gradually falling till the week 12 --> then it stabilizes till term.
But PPBS shows sharper, more sustained rise, along with rising insulin levels!
4) This is why Uptodate defines GDM as a pregnancy with abnormal glucose tolerance in the 2nd or 3rd trimester of pregnancy --> if present earlier or in the 1st trimester --> its overt DM.
A formal evaluation is done in the nonpregnant state for a confirmed dx.
A formal evaluation is done in the nonpregnant state for a confirmed dx.
5) As you can see, GDM is a feature of the latter half of pregnancy --> with criteria to differentiate between normal and abnormal.
These criteria are themselves controversial and macrosomia may occur even with normoglycemia.
ncbi.nlm.nih.gov/pmc/articles/P…
These criteria are themselves controversial and macrosomia may occur even with normoglycemia.
ncbi.nlm.nih.gov/pmc/articles/P…
6) But we will leave this for the obgyn people to ponder.
We have a simple question -->
Why is pregnancy diabetogenic?
If so, why is there fasting hypoglycemia with postprandial hyperglycemia?
What is the evolutionary basis?
We have a simple question -->
Why is pregnancy diabetogenic?
If so, why is there fasting hypoglycemia with postprandial hyperglycemia?
What is the evolutionary basis?
7) Evolution sees mothers and fathers as partners in so far as their respective goals are met --> to transfer one half of the genome to their offspring.
The same mother might have different offspring with different fathers --> so she will try to ensure equitable resources.
The same mother might have different offspring with different fathers --> so she will try to ensure equitable resources.
8) But this is not enough for the fetus --> since his 'siblings' might originate from different fathers --> he sees them as direct competition.
He tries to game the system --> to take more from the mother!
The mother and fetus are thus at war!
He tries to game the system --> to take more from the mother!
The mother and fetus are thus at war!
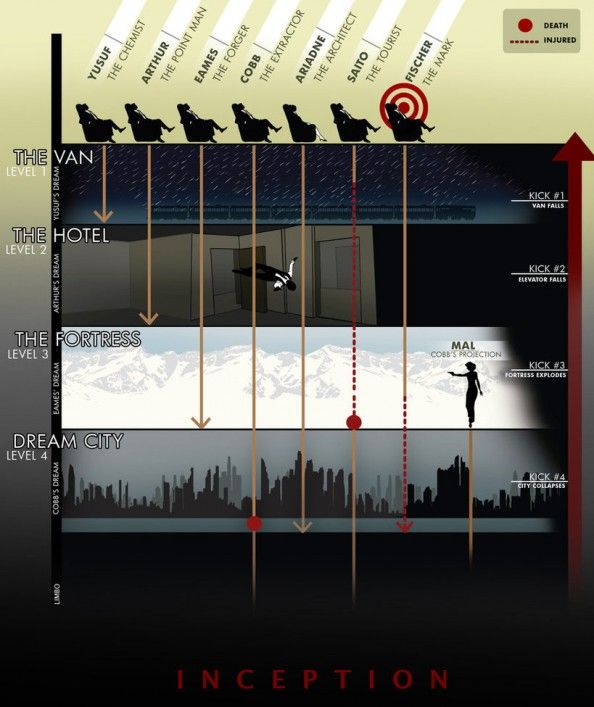
9) These revolutionary ideas were proposed by Robert Trivers (L) and David Haig (R) in the 1970s and 80s.


10) I have provided this article as a basic introduction to the concept of maternal-fetal conflict.
aeon.co/essays/why-pre…
aeon.co/essays/why-pre…
11) The next question is --> how does this fetomaternal conflict take place in the context of blood glucose?
It is basically a battle of hormones.
Maternal insulin vs fetal human placental lactogen (hPL), human placental GH (hPGH), hGH, progesterone and glucocorticoids.
It is basically a battle of hormones.
Maternal insulin vs fetal human placental lactogen (hPL), human placental GH (hPGH), hGH, progesterone and glucocorticoids.
12) Blood sugar transport across the placental membrane is proportiona to maternal blood sugar levels.
The mother tries to prevent excess sugar from flowing to the fetus --> using insulin!
The fetus secretes these diabetogenic hormones to counteract this insulin!
The mother tries to prevent excess sugar from flowing to the fetus --> using insulin!
The fetus secretes these diabetogenic hormones to counteract this insulin!
13) Its an arms race --> with each side upping the ante.
If the mother wins --> its euglycemia and a normal pregnancy.
If the fetus wins --> excess sugar flows into the fetus --> fetal hyperinsulinism with hypoglycemia, macrosomia and a host of complications!
If the mother wins --> its euglycemia and a normal pregnancy.
If the fetus wins --> excess sugar flows into the fetus --> fetal hyperinsulinism with hypoglycemia, macrosomia and a host of complications!
14) Now the real fun part --> what is the proof?
We will begin with the evidence that correlates with our theory.
As you can see, these hormones rise to their peak toward term --> when risk of GDM is maximum!
We will begin with the evidence that correlates with our theory.
As you can see, these hormones rise to their peak toward term --> when risk of GDM is maximum!


15) hPL is almost completely independent of maternal control --> it is constitutively expressed by the placenta --> acute hypo or hyperglycemia don't alter its concentration.
This is expected ---> you wouldn't expect the fetus to expose its weaponry to the mother!
This is expected ---> you wouldn't expect the fetus to expose its weaponry to the mother!
16) Human growth hormones (hGH) acts through both GH and PRL receptors.
In fact, both GH and PRL have certain actions in common --> induce lipolysis and insulin resistance (IR).
It is believed that these actions of GH actually take place through PRL receptors.
In fact, both GH and PRL have certain actions in common --> induce lipolysis and insulin resistance (IR).
It is believed that these actions of GH actually take place through PRL receptors.
18) hPL has nearly 87% common with hGH --> in fact it differs only in those areas which mediate binding to GH receptors .
So it binds only to PRL receptors but not GH receptors.
Other mammalian placental lactogens are derived from duplication of the PRL gene!
So it binds only to PRL receptors but not GH receptors.
Other mammalian placental lactogens are derived from duplication of the PRL gene!
19) In short, the insulin resistance and lipolytic action of GH is mediated through PRL --> and hPL acts through PRL receptors and is itself a duplicate of the PRL gene --> its basically prolactin!
20) GH induces acute hyperglycemia via gluconeogenesis but at the same time it induces lipolysis --> increased FFA and ketogenesis --> promotes IR --> shifts metabolism from glucose to fat! (via ketoacids)
This frees up maternal glucose for the fetus!
This frees up maternal glucose for the fetus!
21) Thus, 3rd trimester pregnancies --> more sugar and ketones than 1st trimester or nonpregnant women!
Who does this?
hPL acting as prolactin acting as growth hormone!
Hormoneception!
Who does this?
hPL acting as prolactin acting as growth hormone!
Hormoneception!
22) The next proof involves --> human placental growth hormone aka hPGH --> like hPL it reaches maximal levels at term --> nearly 85% of the biologic GH activity of maternal blood at that time --> hPGH.
Unlike hGH it is not suppressible by IGF-1!
Unlike hGH it is not suppressible by IGF-1!
23) The human pancreatic islets hypertrophy in pregnancy --> supplying increased maternal insulin!
This is an article for reference!
ncbi.nlm.nih.gov/pmc/articles/P…
This is an article for reference!
ncbi.nlm.nih.gov/pmc/articles/P…
24) The placenta contains enzymes that degrade insulin and also acts as a 'sink' for insulin --> with a large no of insulin receptors that either don't function or have an antagonistic action wrt insulin!
The pancreas tricks insulin to act against itself!
The pancreas tricks insulin to act against itself!
25) If you are with me this far, then you will have noticed that I have provided very few references as I didn't want to clutter up the Tweetorial.
I have used David Haig's own work for this deep dive.
You will find a century's worth of references here.
jstor.org/stable/3037249…
I have used David Haig's own work for this deep dive.
You will find a century's worth of references here.
jstor.org/stable/3037249…
26) I have also used these reference books --> to provide certain clinical details!
27) So it seems to be pretty cut and dried by now.
But that isn't the way of evolution.
It would seem pretty clear by now that human pregnancies won't survive without hPL.
But that isn't the way of evolution.
It would seem pretty clear by now that human pregnancies won't survive without hPL.
28) That is how it should be.
But it isn't so.
There have been several successful pregnancies with a COMPLETE LACK OF HPL or HPGH.
pubmed.ncbi.nlm.nih.gov/9490304/
But it isn't so.
There have been several successful pregnancies with a COMPLETE LACK OF HPL or HPGH.
pubmed.ncbi.nlm.nih.gov/9490304/
29) This seems to suggest that these hormones, even though present in large amounts have only a marginal role to play.
It is more likely that the usual suspects like cortisol and progesterone are the actual culprits.
Perhaps the real story will come out with more research!
It is more likely that the usual suspects like cortisol and progesterone are the actual culprits.
Perhaps the real story will come out with more research!
30) Thank you for accompanying me on this fantastic journey!
Evolutionary medicine is a fascinating science and I hope you have enjoyed this Tweetorial as much as I have enjoyed penning it!
Please share and retweet if you find it informative!
#MedTwitter
Evolutionary medicine is a fascinating science and I hope you have enjoyed this Tweetorial as much as I have enjoyed penning it!
Please share and retweet if you find it informative!
#MedTwitter
Placental invasion of the uterus, via trophoblasts --> provides low resistance high flow channels --> for flow of nutrient rich blood.
Lack of successful invasion --> placental hypoperfusion --> release of vasoconstrictors from placenta --> to squeeze maternal circulation!
Lack of successful invasion --> placental hypoperfusion --> release of vasoconstrictors from placenta --> to squeeze maternal circulation!
This aims to raise maternal MAP and maintain placental perfusion.
This is pre eclampsia +/- IUGR.
As you can see all these things are intimately related at the FM interface!
I will create more Tweetorials explaining these things!
This is pre eclampsia +/- IUGR.
As you can see all these things are intimately related at the FM interface!
I will create more Tweetorials explaining these things!
• • •
Missing some Tweet in this thread? You can try to
force a refresh