
How long is long enough?🤔
I channeled my inner @BradSpellberg to give this talk on duration of therapy at the #ThreeRiversASP2022
Interested? Follow the 🧵 below
Not interested? Go Rx a zpak for a cold
#IDtwitter #MedTwitter #MedEd #pharmed #shorterisbetter
I channeled my inner @BradSpellberg to give this talk on duration of therapy at the #ThreeRiversASP2022
Interested? Follow the 🧵 below
Not interested? Go Rx a zpak for a cold
#IDtwitter #MedTwitter #MedEd #pharmed #shorterisbetter


Common question I get as an ID doc relates to duration of abx therapy
How do I decide?
Back in 2010, @PaulSaxMD revealed the secret "5/7 rule" in his @JWatch blog, causing panic in the ID community - Will we still get consults since our secret sauce was revealed??
How do I decide?
Back in 2010, @PaulSaxMD revealed the secret "5/7 rule" in his @JWatch blog, causing panic in the ID community - Will we still get consults since our secret sauce was revealed??


Ok so maybe we have come a long way since then with selecting durations (and consult volume has been fine, phew)
But why do we ❤ a 7 day week to define courses of abx therapy?🤔
Do seven 24 hr intervals of abx exposure have some biologic bacteria busting properties?
But why do we ❤ a 7 day week to define courses of abx therapy?🤔
Do seven 24 hr intervals of abx exposure have some biologic bacteria busting properties?
Well, the 1st question to ask is "What is time?"
You see, "time" is a human construct with no physical properties
We measure days/months/years based on astronomical objects
But what is a week based on?
Uh, it is 7 days because some rich white guy said so a long time ago
You see, "time" is a human construct with no physical properties
We measure days/months/years based on astronomical objects
But what is a week based on?
Uh, it is 7 days because some rich white guy said so a long time ago

So if we can come together and get behind #deletemondays we could ⬇️ global abx consumption by 14%!
That arbitrary 14d course for "sepsis NOS" is now just 12 days!
In fact, according to Mr. McGuire, we could also ⬇️ sadness by 50%
Win/win if you ask me
That arbitrary 14d course for "sepsis NOS" is now just 12 days!
In fact, according to Mr. McGuire, we could also ⬇️ sadness by 50%
Win/win if you ask me


Ok so maybe that won't happen
But when we Rx that 7 day abx course for something, why do we tell our patients to complete the entire Rx *even* if they feel better sooner?
Must be evidence based, right? Right? Bueller?
But when we Rx that 7 day abx course for something, why do we tell our patients to complete the entire Rx *even* if they feel better sooner?
Must be evidence based, right? Right? Bueller?

In fact, this message of taking the entire course even if you feel better is everywhere in both the media and #MedEd
If you stop early, you are told the bacteria will mutate and make you sick all over again
Is that true? Where does this dogma come from?
If you stop early, you are told the bacteria will mutate and make you sick all over again
Is that true? Where does this dogma come from?




The origin is hard to pinpoint, but may trace back to a 1945 case series of severe pneumococcal pna
Despite 81% survival (unthinkable pre-abx), 3 relapses weighed heavy on the authors
"The need for continuing tx even after fever & symptoms subside is suggested by the relapses"
Despite 81% survival (unthinkable pre-abx), 3 relapses weighed heavy on the authors
"The need for continuing tx even after fever & symptoms subside is suggested by the relapses"

But that was an uncontrolled study from 1945
Surely in the next 80 years we would have data showing that "completing the entire abx course" prevents resistance, right?
Surely in the next 80 years we would have data showing that "completing the entire abx course" prevents resistance, right?

Before we get in the data, it is important to discuss how abx resistance occurs
"Completing the course" helps to prevent 🔸️Target Selection🔸️ -> think TB and HIV
However, 🔸️Collateral Selection🔸️ is much more important with our common infections - think ESKAPE bugs
"Completing the course" helps to prevent 🔸️Target Selection🔸️ -> think TB and HIV
However, 🔸️Collateral Selection🔸️ is much more important with our common infections - think ESKAPE bugs

With collateral selection, LONGER abx exposer causes GREATER pressure to select for resistance
NO trials show shorter tx causes ⬆️ resistance w/ ESKAPE bugs
In fact, RCT data shows shorter tx leads to ⬇️ resistance
So maybe we need better endpoints then "complete the course"
NO trials show shorter tx causes ⬆️ resistance w/ ESKAPE bugs
In fact, RCT data shows shorter tx leads to ⬇️ resistance
So maybe we need better endpoints then "complete the course"

So what does the WHO and CDC have to say about this?
In recent years, they have shifted messaging from "not completing the course can make you sick again" to "listen to your doctor, they know what is best"
Oh really?
So how good are clinicians at choosing abx durations?🤔
In recent years, they have shifted messaging from "not completing the course can make you sick again" to "listen to your doctor, they know what is best"
Oh really?
So how good are clinicians at choosing abx durations?🤔



Turns out, we are terrible
This slide doesn't work as well on twitter as in real life, but just so you know we have made both James Van Der Beek and Michael Jordan cry
This slide doesn't work as well on twitter as in real life, but just so you know we have made both James Van Der Beek and Michael Jordan cry

So what can we do to improve practice?
Learn what the data says about common infections!
@BradSpellberg's website bradspellberg.com/shorter-is-bet… should be bookmarked by every clinician
Let's take a look at some of these disease states 👀
Learn what the data says about common infections!
@BradSpellberg's website bradspellberg.com/shorter-is-bet… should be bookmarked by every clinician
Let's take a look at some of these disease states 👀

Pneumonia 🤧
For CAP, we actually have more data in peds than adults 👶>👩🦳
However, 3-5 days = up to 14 days for both - Paging ATS/IDSA CAP guideline writers📟
Less RCT data in VAP, but typically 7-8d = 10-15d
For CAP, we actually have more data in peds than adults 👶>👩🦳
However, 3-5 days = up to 14 days for both - Paging ATS/IDSA CAP guideline writers📟
Less RCT data in VAP, but typically 7-8d = 10-15d




Cellulitis 👺
Only 4 RCTs, but 5-6d similar to 10-12d
(please don't use levo for cellulitis)
I can't figure out why ESTABLISH-1/2 trials picked 6d Ted vs 10d Lin 🤷♂️
In the Dutch study, 6d group had more obese and recurrent cellulitis pts, which could explain relapse rate
Only 4 RCTs, but 5-6d similar to 10-12d
(please don't use levo for cellulitis)
I can't figure out why ESTABLISH-1/2 trials picked 6d Ted vs 10d Lin 🤷♂️
In the Dutch study, 6d group had more obese and recurrent cellulitis pts, which could explain relapse rate

Complicated UTI 🚽
The definition of a complicated UTI is...well...complicated
Is it pyelo? UTI w/ systemic sx? Anatomical abnormality?
Whatever it is, 5-7d = 10-21d
Granted this is mostly data in females, but thanks to @Ddrekonja et al. we have 7d data in males
The definition of a complicated UTI is...well...complicated
Is it pyelo? UTI w/ systemic sx? Anatomical abnormality?
Whatever it is, 5-7d = 10-21d
Granted this is mostly data in females, but thanks to @Ddrekonja et al. we have 7d data in males

Intra-abdominal infections 🤮
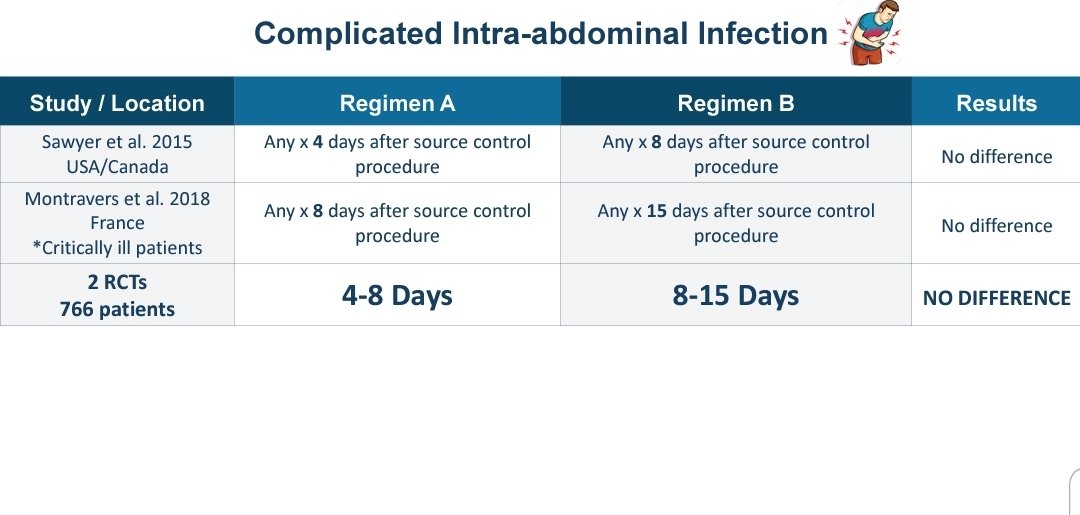
Source control! We have 2 RCTs utilizing that
Everyone's favorite 🛑STOP-IT trial found 4d = waiting 2d after resolution fever/WBC (median 8 days)
In critically ill ICU pts, 8d=15
Source control! We have 2 RCTs utilizing that
Everyone's favorite 🛑STOP-IT trial found 4d = waiting 2d after resolution fever/WBC (median 8 days)
In critically ill ICU pts, 8d=15
COPD 😤 and Acute sinusitis 👃
If you are like me, you just don't give abx to non-severe AECOPD if low procalcitonin
If you do give abx, at least have the decency to stop at no more than 5d - and a cool new study showing maybe just 2d!
For sinusitis, also stop at 5d please
If you are like me, you just don't give abx to non-severe AECOPD if low procalcitonin
If you do give abx, at least have the decency to stop at no more than 5d - and a cool new study showing maybe just 2d!
For sinusitis, also stop at 5d please


Osteo 🦴
Native vertebral OM or DFO w/o surgery? 6wk = 12wk
Can we go shorter?
4wk = 6wk after implant removal ⚒
Shorter?
Pilate RCT found 3wk = 6wk for residual OM in DFO after debridement (same group found 10d=21d for DFI w/o OM, and doing a larger RCT for both)
Native vertebral OM or DFO w/o surgery? 6wk = 12wk
Can we go shorter?
4wk = 6wk after implant removal ⚒
Shorter?
Pilate RCT found 3wk = 6wk for residual OM in DFO after debridement (same group found 10d=21d for DFI w/o OM, and doing a larger RCT for both)



GNR bacteremia 🦠
RCT data mostly enterobacterales, and 7d=14d (source control too)
The swiss study also had a 3rd group that was treated until 75% decline in CRP, which had a median of 7d anyway
I threw in some retrospective data for Pseudomonas just for fun
RCT data mostly enterobacterales, and 7d=14d (source control too)
The swiss study also had a 3rd group that was treated until 75% decline in CRP, which had a median of 7d anyway
I threw in some retrospective data for Pseudomonas just for fun


Running low on tweet space, so here are slides on septic arthritis (2wk=4wk, but mostly small joints in the hand), febrile neutropenia, and squeezed in some parasite love 🦟



Finishing with how we've approached this @AHNtoday thru our excellent ASP group to ⬇️ abx duration for common infections
Shout outs to @TomWalshMD13 @NateShivelyMD @CessnaPharmD @dnbrems @DustinRCarr @cbuchananpharm @c_hoff2 @Wx2_IDPharmD @angelarxmorelli just to name a few
Shout outs to @TomWalshMD13 @NateShivelyMD @CessnaPharmD @dnbrems @DustinRCarr @cbuchananpharm @c_hoff2 @Wx2_IDPharmD @angelarxmorelli just to name a few




So for many common infections, shorter=longer
But by reducing the risk of collateral resistance selection, $, ADRs, DDIs ▶️ shorter is BETTER
We need to move beyond telling pts to take the entire Rx course even if they feel better, and utilize better end points
But by reducing the risk of collateral resistance selection, $, ADRs, DDIs ▶️ shorter is BETTER
We need to move beyond telling pts to take the entire Rx course even if they feel better, and utilize better end points

• • •
Missing some Tweet in this thread? You can try to
force a refresh


