
[1] #Hemodynamics Tweetorial #2
Heart failure pt in ICU is -3.5L after 2d of aggressive diuresis. On day 3, urine output is ⬇️and BUN/Cr is ⬆️
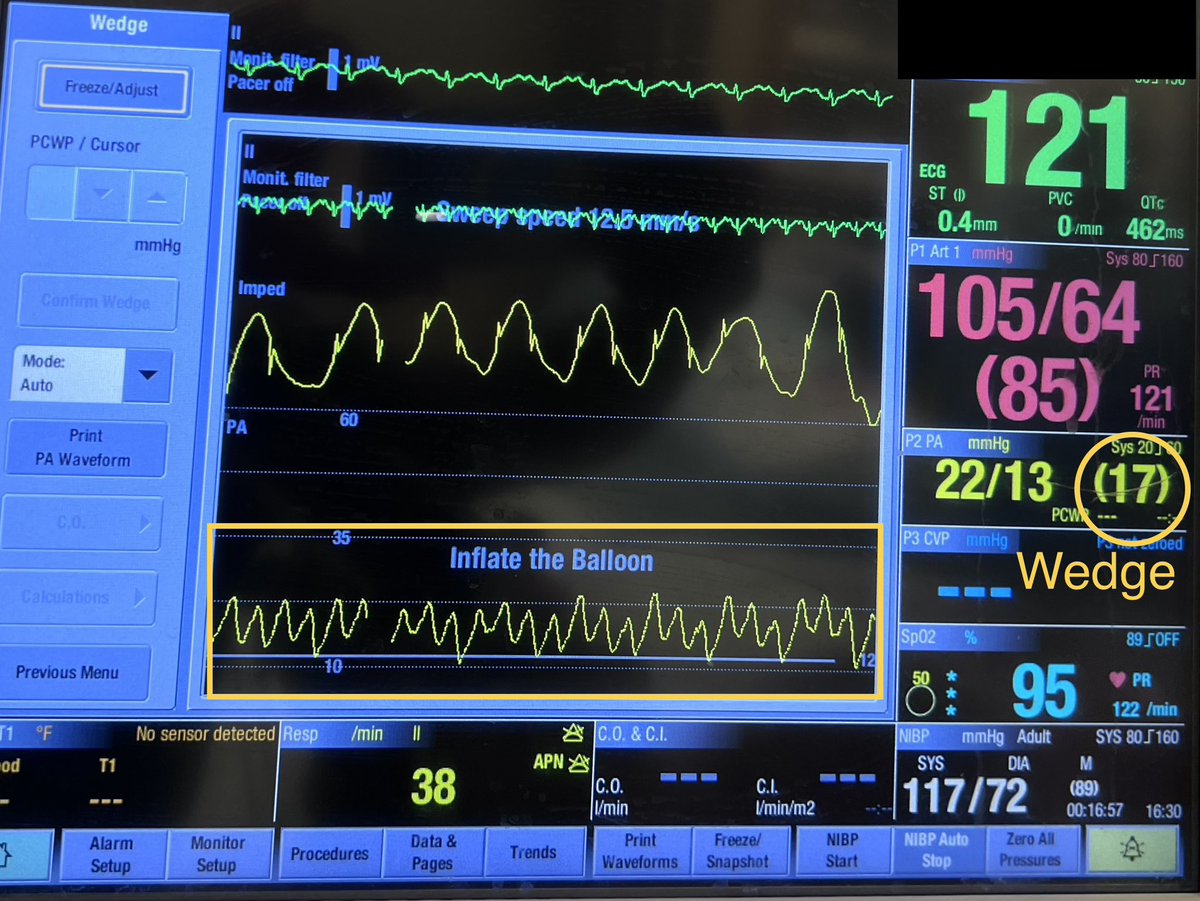
You personally wedge #PAC at bedside and obtain a mean wedge 17 mmHg (a normal mean wedge is 6-10 mmHg). Admission wedge was 24
Heart failure pt in ICU is -3.5L after 2d of aggressive diuresis. On day 3, urine output is ⬇️and BUN/Cr is ⬆️
You personally wedge #PAC at bedside and obtain a mean wedge 17 mmHg (a normal mean wedge is 6-10 mmHg). Admission wedge was 24
[2]
Question 1. Based on wedge 17 mm Hg (good waveform; no trick), you:
Question 1. Based on wedge 17 mm Hg (good waveform; no trick), you:
[3]
Before you use the pulmonary artery catheter #PAC information, you should know its pitfalls
Given the potential impact of #PAC-related decisions, consider learning as much (or more) as the ICU nurse/cath lab tech about #PAC setup and troubleshooting
Before you use the pulmonary artery catheter #PAC information, you should know its pitfalls
Given the potential impact of #PAC-related decisions, consider learning as much (or more) as the ICU nurse/cath lab tech about #PAC setup and troubleshooting
[4]
🔹”Zeroing”
🔹”Leveling”
🔹”Damping”
🔹”Zeroing”
🔹”Leveling”
🔹”Damping”
[5]
🔹”Zeroing”
-Device is “zeroed” to open the air-fluid interface to atmospheric pressure (AP)
-AP is the reference standard against which other pressures are measured
-“Re-zeroing” is done often since transducer and atmospheric pressure drift away from calibration point
🔹”Zeroing”
-Device is “zeroed” to open the air-fluid interface to atmospheric pressure (AP)
-AP is the reference standard against which other pressures are measured
-“Re-zeroing” is done often since transducer and atmospheric pressure drift away from calibration point
[6]
Transducer components and directions of the components 👇🏻
Transducer components and directions of the components 👇🏻

[7]
To zero:
-Point the 3-way stopcock “off” towards the patient (points up on the transducer)
-This now allows the vent port to be “opened” to atmospheric pressure
-If vent port cap is not fenestrated, it has to be temporarily removed
(port cap in video 👇🏻 is fenestrated)
To zero:
-Point the 3-way stopcock “off” towards the patient (points up on the transducer)
-This now allows the vent port to be “opened” to atmospheric pressure
-If vent port cap is not fenestrated, it has to be temporarily removed
(port cap in video 👇🏻 is fenestrated)
[9]
🔹”Leveling”
-Selection of a point of interest (R atrium for #PAC) at which the ref standard (zero) is set
-RA is considered the phlebostatic axis (RA is also used as the ref point for CVP assessm)
*REMEMBER:
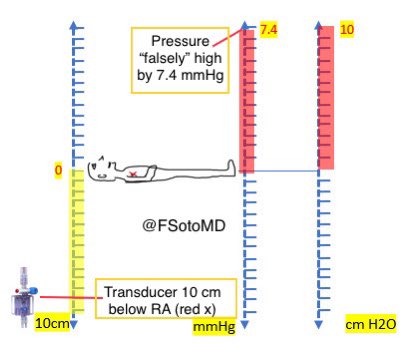
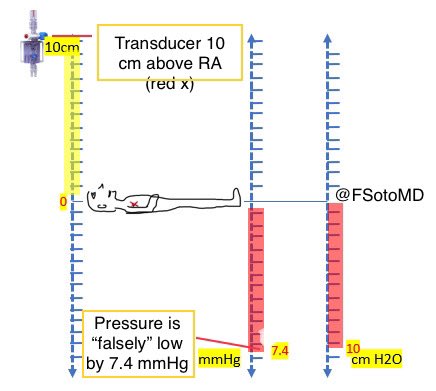
Pressure changes 7.4mmHg for every 10 cm transd is ⬆️ or ⬇️ RA
🔹”Leveling”
-Selection of a point of interest (R atrium for #PAC) at which the ref standard (zero) is set
-RA is considered the phlebostatic axis (RA is also used as the ref point for CVP assessm)
*REMEMBER:
Pressure changes 7.4mmHg for every 10 cm transd is ⬆️ or ⬇️ RA
[10]
To level:
Identify the point at which the:
🔹mid-axillary line intersects with the
🔹4th intercostal space
That point should be at the same level of the transducer’s diaphragm
Consider using an accurate leveling system (e.g., laser) to match transducer ht with RA ht
To level:
Identify the point at which the:
🔹mid-axillary line intersects with the
🔹4th intercostal space
That point should be at the same level of the transducer’s diaphragm
Consider using an accurate leveling system (e.g., laser) to match transducer ht with RA ht

[11]
Leveling is 🔑
🔷IN RELATIONSHIP TO TRANSDUCER:
🔹For every 10cm that RA “rises” above transducer, pressure falsely “rises” 7.4 mmHg
🔹For every 10cm that RA is “lowered” below transducer, pressure falsely “lowers” 7.4 mmHg
—
RA ⬆️ = pressure ⬆️
RA ⬇️= pressure ⬇️
Leveling is 🔑
🔷IN RELATIONSHIP TO TRANSDUCER:
🔹For every 10cm that RA “rises” above transducer, pressure falsely “rises” 7.4 mmHg
🔹For every 10cm that RA is “lowered” below transducer, pressure falsely “lowers” 7.4 mmHg
—
RA ⬆️ = pressure ⬆️
RA ⬇️= pressure ⬇️

[12]
Answer to Question 1 is: “Can I trust that wedge?”
In our case, when wedge 17 mmHg was obtained, transducer wasn’t leveled and pt’s RA was about 11 cm above the transducer.
Therefore, real wedge was <10 mmHg.
Diuresis was held for a few hrs and restarted at home dose
Answer to Question 1 is: “Can I trust that wedge?”
In our case, when wedge 17 mmHg was obtained, transducer wasn’t leveled and pt’s RA was about 11 cm above the transducer.
Therefore, real wedge was <10 mmHg.
Diuresis was held for a few hrs and restarted at home dose
BONUS:
If you see pressure tracings that become negative (below Zero), consider an unaddressed LEVELING issue before you interpret and use that #PAC info
See 👇🏻 RAP tracing: transducer was higher than RA level, causing sub-Zero values (RA level is ⬇️ = pressure is “falsely” ⬇️)
If you see pressure tracings that become negative (below Zero), consider an unaddressed LEVELING issue before you interpret and use that #PAC info
See 👇🏻 RAP tracing: transducer was higher than RA level, causing sub-Zero values (RA level is ⬇️ = pressure is “falsely” ⬇️)
[13]
🔹”Damping”
Damping is the “shock absorber” effect on the pressure line (like a car suspension)
Overdamping:
Sluggish oscillations
Underdamping:
Oscillations are too pronounced
Causes of Over and Under-Damping 👇🏻
🔹”Damping”
Damping is the “shock absorber” effect on the pressure line (like a car suspension)
Overdamping:
Sluggish oscillations
Underdamping:
Oscillations are too pronounced
Causes of Over and Under-Damping 👇🏻


[14]
Which answer is FALSE regarding an OVERDAMPED waveform
Which answer is FALSE regarding an OVERDAMPED waveform
[15]
🔹OVER-damping
🔸Slurred upstroke
🔸ABSENT Dicrotic Notch
🔸Systolic is Underestimated
🔸Diastolic is Overestimated
🔸MAP is usually preserved
🔸Pulse pressure is underestimated (affects PAPi calc)
🔸The waveform gets “squished” (think letter “O” for “O”verdamped)
🔹OVER-damping
🔸Slurred upstroke
🔸ABSENT Dicrotic Notch
🔸Systolic is Underestimated
🔸Diastolic is Overestimated
🔸MAP is usually preserved
🔸Pulse pressure is underestimated (affects PAPi calc)
🔸The waveform gets “squished” (think letter “O” for “O”verdamped)


[17]
Which answer is FALSE regarding an UNDERDAMPED waveform:
Which answer is FALSE regarding an UNDERDAMPED waveform:
[18]
🔹UNDER-damping
🔸Non-physiologic oscillations during Diast phase
🔸Deep dicrotic notch
🔸Systolic is Overestimated
🔸Diastolic is Underestimated
🔸Pulse pressure overestimation
🔸MAP is usually preserved
🔸Waveform gets “stretched out” (inverted “U” for “U”nderdamped”
🔹UNDER-damping
🔸Non-physiologic oscillations during Diast phase
🔸Deep dicrotic notch
🔸Systolic is Overestimated
🔸Diastolic is Underestimated
🔸Pulse pressure overestimation
🔸MAP is usually preserved
🔸Waveform gets “stretched out” (inverted “U” for “U”nderdamped”


[20]
Besides looking at the waveforms, consider FAST-FLUSH test (square wave test) to assess for waveform damping characteristics
🔸Hold fast-flush device for <1 sec
🔸Assess the square wave and characteristics of the wave (s) that follow
See image 👇🏻
Besides looking at the waveforms, consider FAST-FLUSH test (square wave test) to assess for waveform damping characteristics
🔸Hold fast-flush device for <1 sec
🔸Assess the square wave and characteristics of the wave (s) that follow
See image 👇🏻

[21]
TAKE-HOME Messages (applies to ICU and outpt cardiac/PH pts)
🔷Before you interpret/use #PAC info, verify:
🔸Zeroing (atmosp pressure)
🔸Leveling (match transducer level to RA, AKA phlebostatic axis)
🔸Waveforms (to exclude OVER or UNDER damping affecting actual values)
TAKE-HOME Messages (applies to ICU and outpt cardiac/PH pts)
🔷Before you interpret/use #PAC info, verify:
🔸Zeroing (atmosp pressure)
🔸Leveling (match transducer level to RA, AKA phlebostatic axis)
🔸Waveforms (to exclude OVER or UNDER damping affecting actual values)
TAKE-HOME Messages 2
🔸If you see -ve (below Zero) pressures, especially in non-ill pts, consider leveling error
🔸Over and Underdamping affect Syst and Diast pressures; MAP is usually preserved
🔸Verify line flushing/waveform every time a MVsat is drawn from distal #PAC port
🔸If you see -ve (below Zero) pressures, especially in non-ill pts, consider leveling error
🔸Over and Underdamping affect Syst and Diast pressures; MAP is usually preserved
🔸Verify line flushing/waveform every time a MVsat is drawn from distal #PAC port
Additional relevant reading:
-NEJM Art Line Pressure Transducer
nejm.org/doi/full/10.10…
-Deranged physiology
derangedphysiology.com/main/cicm-prim…
-NEJM Art Line Pressure Transducer
nejm.org/doi/full/10.10…
-Deranged physiology
derangedphysiology.com/main/cicm-prim…
#MedEd
#MedTwitter
#hemodynamics
#Cardiotwitter
#PAC
#RHC
@PulmPEEPs @IM_Crit_ @CardioNerds @iceman_ex @msiuba @Thind888 @OrlandoRPN @AHajduczok @robmentz @RyanTedfordMD @AndrewJSauer @nickmmark @RichardAFerraro @GallodeMoraesMD
#MedTwitter
#hemodynamics
#Cardiotwitter
#PAC
#RHC
@PulmPEEPs @IM_Crit_ @CardioNerds @iceman_ex @msiuba @Thind888 @OrlandoRPN @AHajduczok @robmentz @RyanTedfordMD @AndrewJSauer @nickmmark @RichardAFerraro @GallodeMoraesMD
• • •
Missing some Tweet in this thread? You can try to
force a refresh



