1) There are many books on clinical medicine and most of them are horrible.
Here is my curated list.
The first and most important book has to be Dr. Boloor's text.
Well written and compiled, it has all the little snippets that Indian examiners love.
Best Indian book imo.
Here is my curated list.
The first and most important book has to be Dr. Boloor's text.
Well written and compiled, it has all the little snippets that Indian examiners love.
Best Indian book imo.

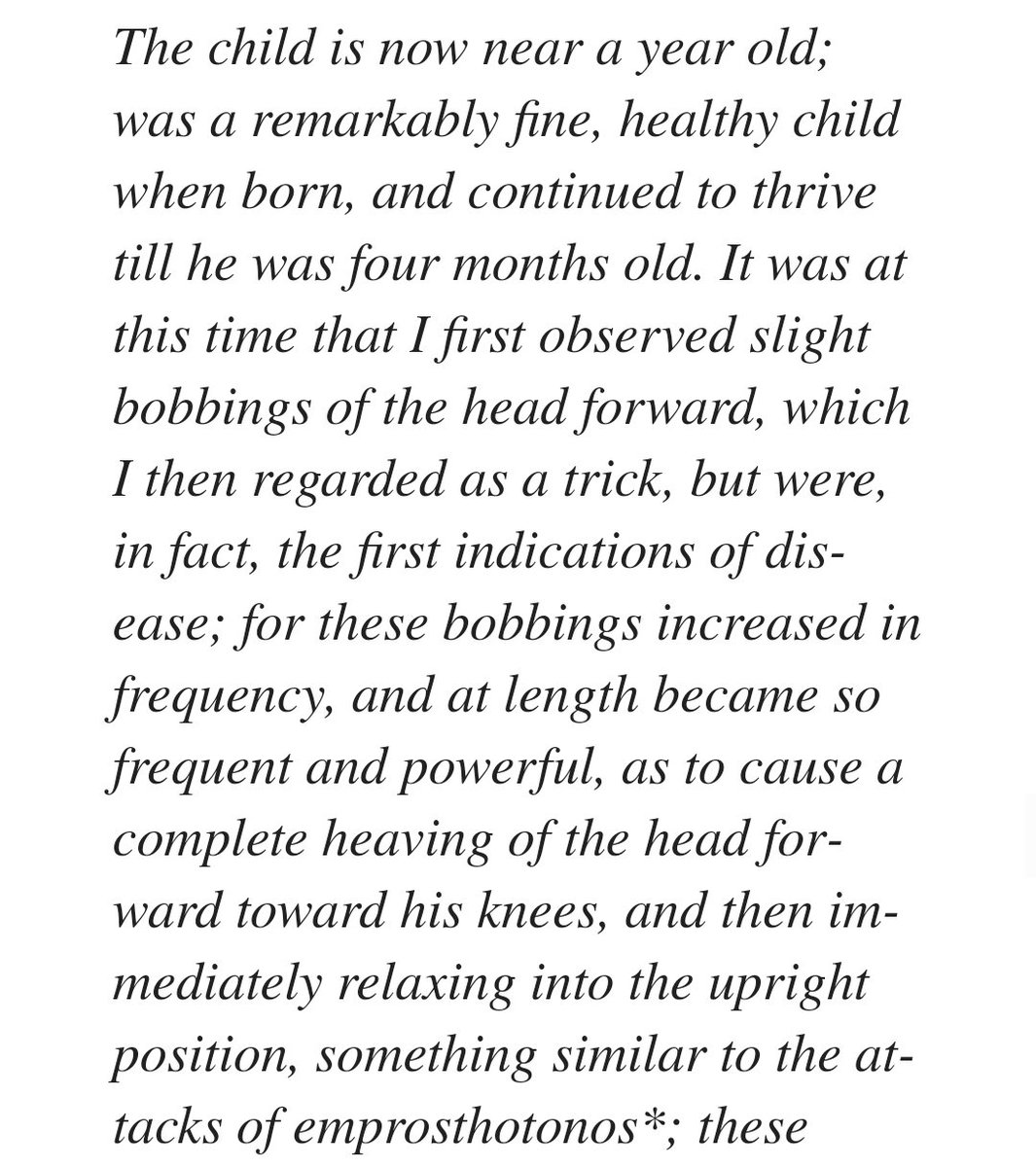
2) The book for the discerning internist.
You will love this if you are into medical history.
This is not for beginners since it often delves deep into stuff that have little knowledge of, YET!
You will love this if you are into medical history.
This is not for beginners since it often delves deep into stuff that have little knowledge of, YET!

3) A trusty guide.
This is best oriented for UG students though.
It is small, handy and no nonsense but lacks the trivia and snippets that you need for Indian exams, like coin percussion amd whispering pectoriloquy.
This is best oriented for UG students though.
It is small, handy and no nonsense but lacks the trivia and snippets that you need for Indian exams, like coin percussion amd whispering pectoriloquy.
4) The new edition isn't that good.
The explanations are succint but it has been overloaded with approach to investigations.
Please avoid unless you really like it.
The explanations are succint but it has been overloaded with approach to investigations.
Please avoid unless you really like it.

5) This is an underrated gem.
Most Indian students don't use this.
Its pretty darn comprehensive and has very clear explanations.
Let me know what you think.
Most Indian students don't use this.
Its pretty darn comprehensive and has very clear explanations.
Let me know what you think.
6) A book that does not know what it wants to do.
It is so overloaded with data that it causes cognitive overloading.
It is a good reference but otherwise entirely avoidable.
It is so overloaded with data that it causes cognitive overloading.
It is a good reference but otherwise entirely avoidable.

7) Not for medicine PG if you are serious about it.
The case based approach works for some but the questions here are too simplistic.
It also lacks a proper structure.
I can only recommend this for UG students but even they are using Boloor nowadays.
The case based approach works for some but the questions here are too simplistic.
It also lacks a proper structure.
I can only recommend this for UG students but even they are using Boloor nowadays.

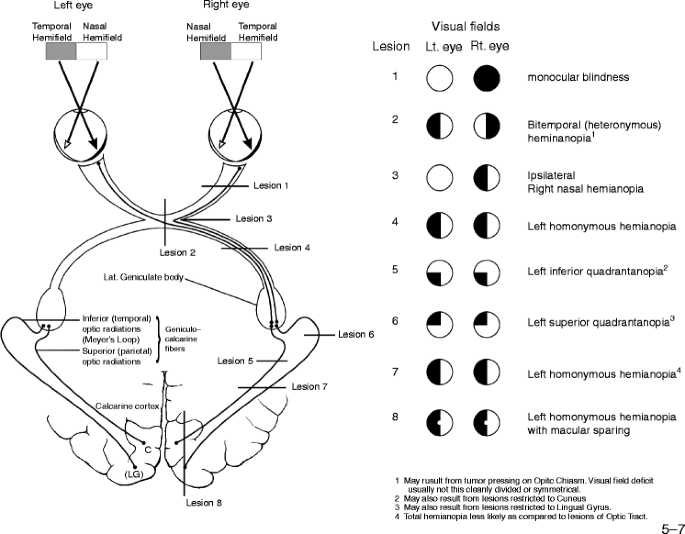
8) This was my go to book for neuro as a resident.
https://twitter.com/AdiG1993/status/1547973504360136705?t=xVv7yI_Dl5yFGExCnVRfdw&s=19
9) A great book especially for those who are disinclined towards neuro.
You will have to pass the exams and neuro is often the long case.
Use this handy guide for easy comprehension and an approach towards the common cases in the wards.
You will have to pass the exams and neuro is often the long case.
Use this handy guide for easy comprehension and an approach towards the common cases in the wards.

10) This is my PERSONAL recommendation.
I have gone through all of them and stand by my opinions.
Please feel free to provide your own in the comments below!
#MedTwitter
#clinicalmedicine
#books
#residency
I have gone through all of them and stand by my opinions.
Please feel free to provide your own in the comments below!
#MedTwitter
#clinicalmedicine
#books
#residency
• • •
Missing some Tweet in this thread? You can try to
force a refresh