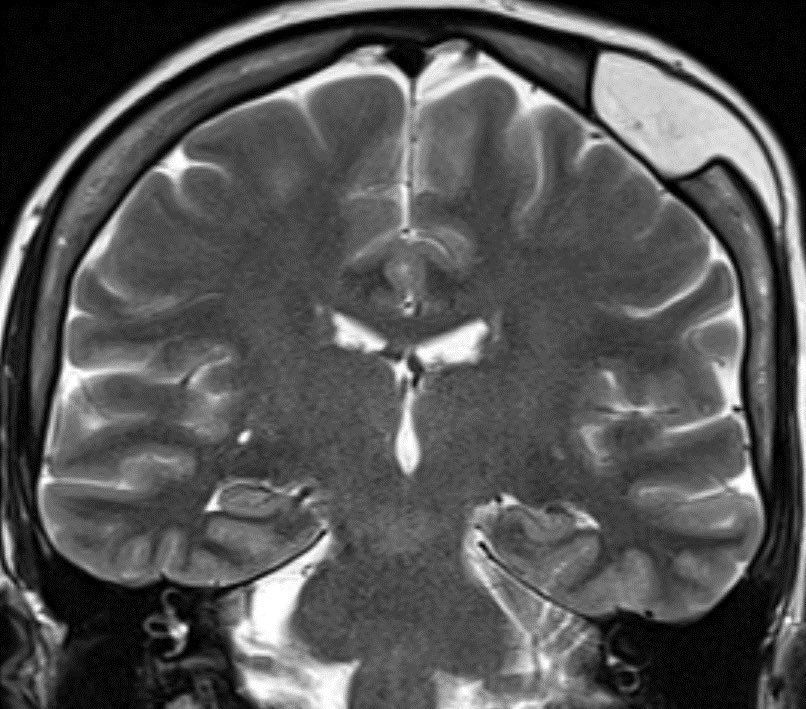
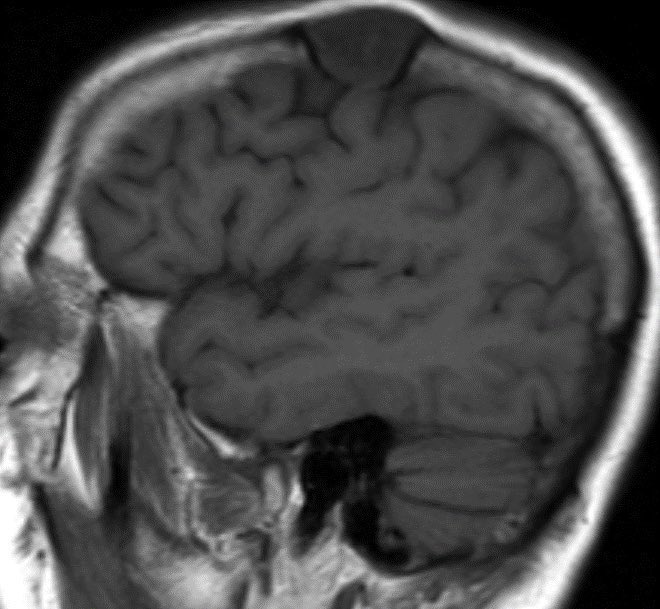
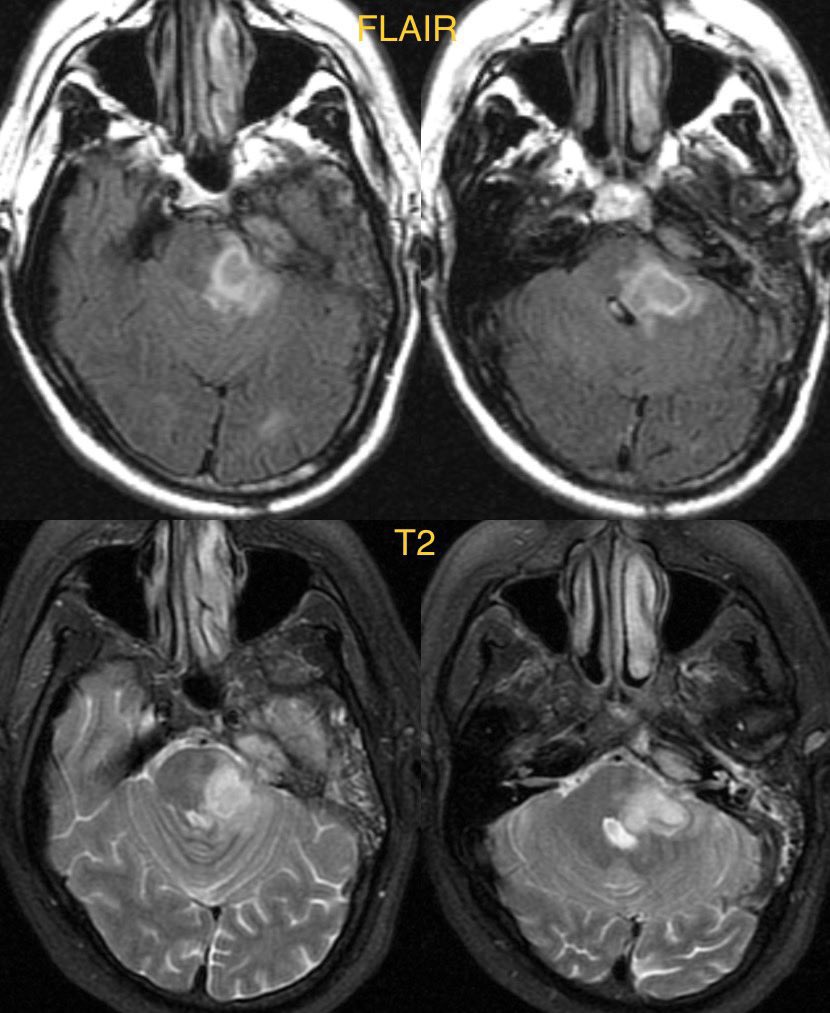
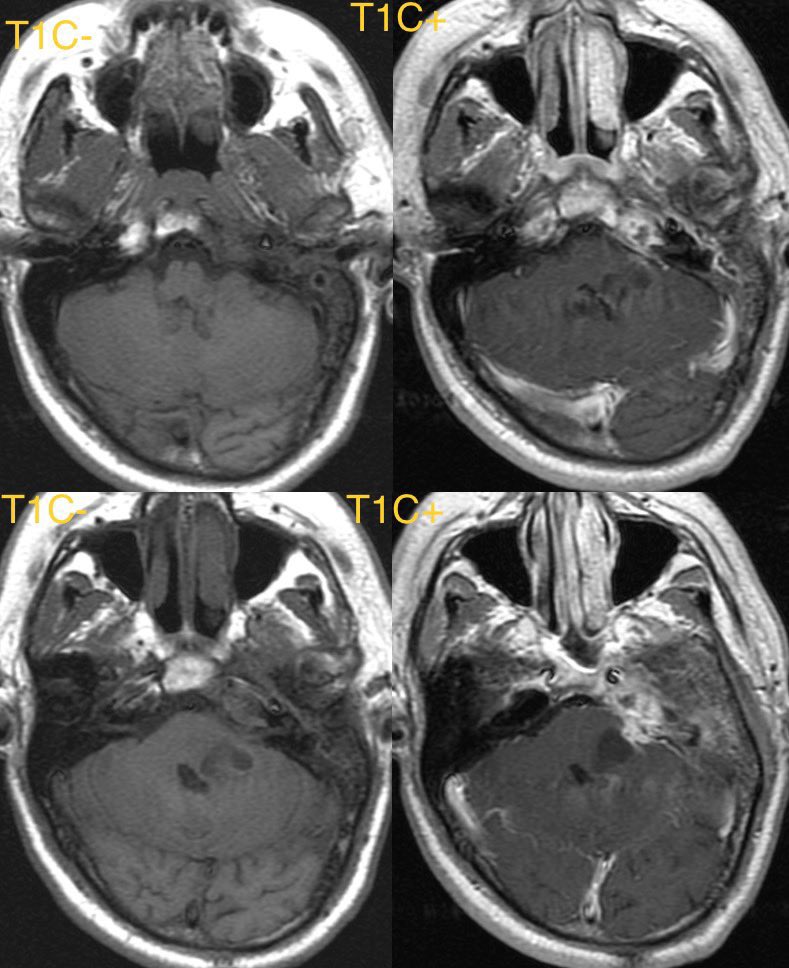
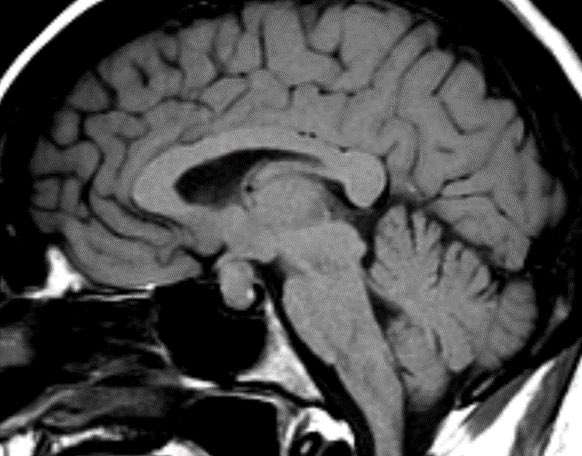
Patient with history of melanoma on ipilimumab. MR shows homogenously enhancing bulbous enlargement of the pituitary gland with thickened stalk.
#radres #neurorad #futureradres #Neurology @TheASNR @ESNRad @ARRS_Radiology
#radres #neurorad #futureradres #Neurology @TheASNR @ESNRad @ARRS_Radiology


Differential Diagnosis:
Pituitary macroadenoma
Lymphocytic hypophysitis
Granulomatous disease
Craniopharyngioma (papillary type)
Pituitary macroadenoma
Lymphocytic hypophysitis
Granulomatous disease
Craniopharyngioma (papillary type)
Diagnosis: Lymphocytic Hypophysitis
Clinical history is key here as there is an association with ipilimumab. Helpful clues on imaging include a thickened non tapered pituitary stalk with bulbous enlargement of the gland though usually no significant widening of the sella
Clinical history is key here as there is an association with ipilimumab. Helpful clues on imaging include a thickened non tapered pituitary stalk with bulbous enlargement of the gland though usually no significant widening of the sella
• • •
Missing some Tweet in this thread? You can try to
force a refresh