
One of the most important diagnostic tests in Cardiology to interpret is the EKG.
Here are my thoughts and notes. Will continue to this thread. Let me know what you think!
Thread #4: ECG Segments
#arjuncardiology #medtwitter #CardioTwitter #MedEd #IMG
Here are my thoughts and notes. Will continue to this thread. Let me know what you think!
Thread #4: ECG Segments
#arjuncardiology #medtwitter #CardioTwitter #MedEd #IMG
General Principles:
- Positive deflection: wave of depolarization towards positive pole of that lead
- Negative deflection: wave of depolarization towards negative pole of that lead
- Biphasic deflection: wave of depolarization is perpendicular to a lead
- Positive deflection: wave of depolarization towards positive pole of that lead
- Negative deflection: wave of depolarization towards negative pole of that lead
- Biphasic deflection: wave of depolarization is perpendicular to a lead

Normal Sinus P-wave:
- Atrial depolarization that marks spontaneous depolarization of pacemakers cells in the right atrium
- Should be negative P-wave in aVR and upright in lead II
- Can communicate 'sinus rhythm with 1:1 AV conduction'
- Atrial depolarization that marks spontaneous depolarization of pacemakers cells in the right atrium
- Should be negative P-wave in aVR and upright in lead II
- Can communicate 'sinus rhythm with 1:1 AV conduction'
Normal QRS Complex:
- First phase: brief duration and spread of stimulus through interventricular septum (left side is stimulated first through branch of the left bundle of His); then depolarization spreads from LV to RV
- Second phase: Simultaneous stimulation of LV & RV
- First phase: brief duration and spread of stimulus through interventricular septum (left side is stimulated first through branch of the left bundle of His); then depolarization spreads from LV to RV
- Second phase: Simultaneous stimulation of LV & RV

ST Segments:
- Represents early phase of ventricular repolarization (usually isoelectric); slight deviation (<1 mm may be seen normally)
- Can have short ST-segments and T-waves that appear to take off almost from J-point (variant of early repolarization)
- Represents early phase of ventricular repolarization (usually isoelectric); slight deviation (<1 mm may be seen normally)
- Can have short ST-segments and T-waves that appear to take off almost from J-point (variant of early repolarization)

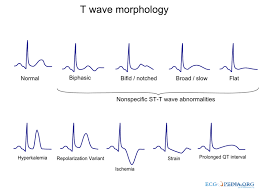
Normal T-waves:
- Ventricular repolarization: return of stimulated muscle to the resting state (ST-segment, T-waves, and U-waves)
- Normally, should follow the direction of the main QRS deflection; should always be negative in aVR and positive in II and generally V4-V6
- Ventricular repolarization: return of stimulated muscle to the resting state (ST-segment, T-waves, and U-waves)
- Normally, should follow the direction of the main QRS deflection; should always be negative in aVR and positive in II and generally V4-V6
Stayed tuned for the next thread! Let me know what you think. Special thanks to these websites for these amazing graphics:
thoracickey.com/understanding-…
cvphysiology.com/Arrhythmias/A0…
litfl.com/j-point-ecg-li…
wikidoc.org/index.php/T_wa…
thoracickey.com/understanding-…
cvphysiology.com/Arrhythmias/A0…
litfl.com/j-point-ecg-li…
wikidoc.org/index.php/T_wa…
• • •
Missing some Tweet in this thread? You can try to
force a refresh










