
One of the most important diagnostic tests in Cardiology to interpret is the EKG.
Here are my thoughts and notes. Will continue to this thread. Let me know what you think!
Thread #5: Axis Deviation
#arjuncardiology #medtwitter #CardioTwitter #MedEd #IMG
Here are my thoughts and notes. Will continue to this thread. Let me know what you think!
Thread #5: Axis Deviation
#arjuncardiology #medtwitter #CardioTwitter #MedEd #IMG
QRS Axis:
- General direction in the frontal plane towards which the QRS complex is predominantly pointed
- General rule: Mean QRS points mid-way b/w any 2 leads that show tall R-wave of equal height
- If depolarization is perpendicular to any lead, will see biphasic complex
- General direction in the frontal plane towards which the QRS complex is predominantly pointed
- General rule: Mean QRS points mid-way b/w any 2 leads that show tall R-wave of equal height
- If depolarization is perpendicular to any lead, will see biphasic complex

Axis Deviation:
- For most people, the axis lies between -30 and + 100 degrees
- Left axis: < -30 degrees, lead II rS pattern (S-wave deeper than R-wave is tall)
- Right axis: > +100 degrees (R-wave in III > II)
- For most people, the axis lies between -30 and + 100 degrees
- Left axis: < -30 degrees, lead II rS pattern (S-wave deeper than R-wave is tall)
- Right axis: > +100 degrees (R-wave in III > II)

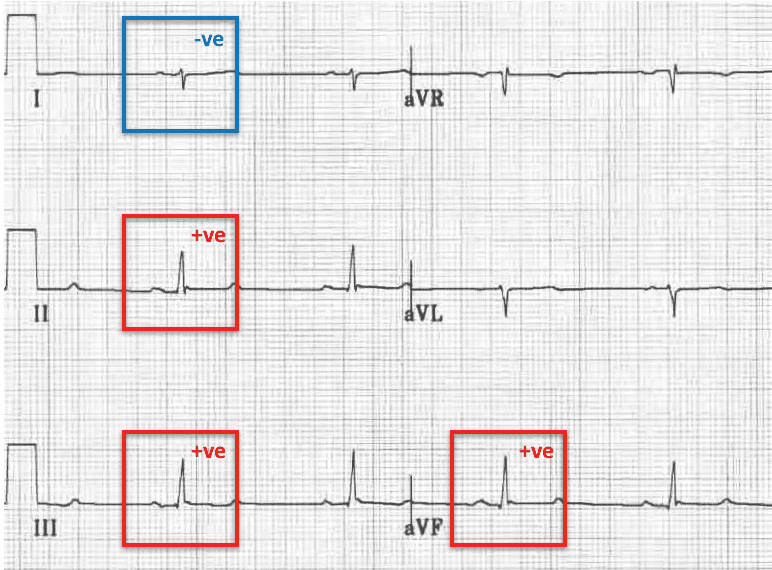
Right-Axis Deviation:
- Seen in RVH
- R-wave in lead III > II
- Can be seen with myocardial infarction of the lateral wall of the LV (loss of normal leftward depolarization forces)
- Left posterior fascicular block is a rarer cause
- Seen with PE or chronic lung disease
- Seen in RVH
- R-wave in lead III > II
- Can be seen with myocardial infarction of the lateral wall of the LV (loss of normal leftward depolarization forces)
- Left posterior fascicular block is a rarer cause
- Seen with PE or chronic lung disease
Mean T-wave Axis:
- Generally points in the same direction as the mean QRS
Left Axis Deviation:
- Can be seen in LVH and left anterior fascicular block
- QRS is positive in lead I (dominant R-wave) and negative in leads II, III, and aVF (dominant S-wave)
- Generally points in the same direction as the mean QRS
Left Axis Deviation:
- Can be seen in LVH and left anterior fascicular block
- QRS is positive in lead I (dominant R-wave) and negative in leads II, III, and aVF (dominant S-wave)

Thanks to these websites for these amazing graphics:
litfl.com/ecg-axis-inter…
unm.edu/~lkravitz/EKG/…
litfl.com/right-axis-dev…
litfl.com/left-axis-devi…
Stay tuned for the next thread and let me know what you think!
litfl.com/ecg-axis-inter…
unm.edu/~lkravitz/EKG/…
litfl.com/right-axis-dev…
litfl.com/left-axis-devi…
Stay tuned for the next thread and let me know what you think!
• • •
Missing some Tweet in this thread? You can try to
force a refresh









