1/THREAD
Ever wonder why fluoroquinolones increase the risk of tendon rupture?
It seems so random that a whole class of antibiotics could cause tendon injuries, but the risk is real.
#medtwitter #tweetorial
Ever wonder why fluoroquinolones increase the risk of tendon rupture?
It seems so random that a whole class of antibiotics could cause tendon injuries, but the risk is real.
#medtwitter #tweetorial

2/
Fluoroquinolones inhibit bacterial function by blocking topoisomerase activity.
They first emerged as an antibiotic class in the 1960s, as byproducts of antimalarial quinine development.
Nalidixic acid = the first quinolone discovered.
pubmed.ncbi.nlm.nih.gov/14056431/
Fluoroquinolones inhibit bacterial function by blocking topoisomerase activity.
They first emerged as an antibiotic class in the 1960s, as byproducts of antimalarial quinine development.
Nalidixic acid = the first quinolone discovered.
pubmed.ncbi.nlm.nih.gov/14056431/

3/
The first report of fluoroquinolone-associated tendinopathy occurred in 1983.
2 renal transplant patients received norfloxacin and subsequently developed achilles tenosynovisitis.
Their symptoms spontaneously resolved w/ cessation of the norfloxacin.
pubmed.ncbi.nlm.nih.gov/6223241/
The first report of fluoroquinolone-associated tendinopathy occurred in 1983.
2 renal transplant patients received norfloxacin and subsequently developed achilles tenosynovisitis.
Their symptoms spontaneously resolved w/ cessation of the norfloxacin.
pubmed.ncbi.nlm.nih.gov/6223241/

4/
Subsequent studies confirmed this association, with an overall odds ratio (OR) of 4.3 for achilles tendinopathy (tendonitis or rupture) resulting from fluoroquinolone use.
Patients on corticosteroids (OR 9.1) or dialysis (OR 20) are at highest risk.
pubmed.ncbi.nlm.nih.gov/23026288/
Subsequent studies confirmed this association, with an overall odds ratio (OR) of 4.3 for achilles tendinopathy (tendonitis or rupture) resulting from fluoroquinolone use.
Patients on corticosteroids (OR 9.1) or dialysis (OR 20) are at highest risk.
pubmed.ncbi.nlm.nih.gov/23026288/


5/
In 2008, on the strength of this evidence, the FDA issued a black box warning for fluoroquinolone-associated tendinopathy.
pubmed.ncbi.nlm.nih.gov/18632714/
In 2008, on the strength of this evidence, the FDA issued a black box warning for fluoroquinolone-associated tendinopathy.
pubmed.ncbi.nlm.nih.gov/18632714/

6/
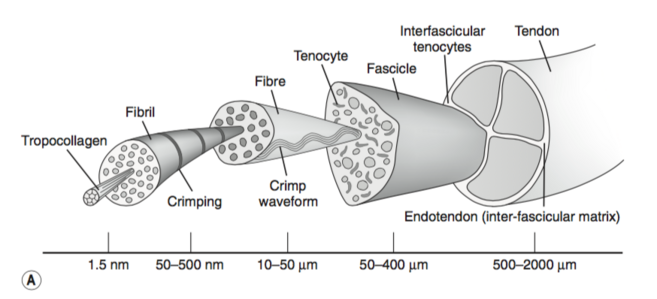
Before we explore mechanisms, let's review tendon structure.
Tendons are composed of collagen fibers surrounded by extracellular matrix (ECM). Tendon-specific fibroblasts called tenocytes produce the collagen and ECM, supporting a tendon' strength.
physio-pedia.com/Tendon_Anatomy
Before we explore mechanisms, let's review tendon structure.
Tendons are composed of collagen fibers surrounded by extracellular matrix (ECM). Tendon-specific fibroblasts called tenocytes produce the collagen and ECM, supporting a tendon' strength.
physio-pedia.com/Tendon_Anatomy
7/
So what are the mechanisms by which fluoroquinolones can injure tendons, or even make them spontaneously rupture?
Theorized answers fall under 3 main categories:
🔑Tenocyte toxicity
🔑Inflammatory responses
🔑⬇️ production and ⬆️ destruction of collagen
So what are the mechanisms by which fluoroquinolones can injure tendons, or even make them spontaneously rupture?
Theorized answers fall under 3 main categories:
🔑Tenocyte toxicity
🔑Inflammatory responses
🔑⬇️ production and ⬆️ destruction of collagen
8/
Let's start w/ impacts on tenocytes.
A 1996 study found that incubation of human tenocytes w/ ciprofloxacin led to increased cell death.
Addition of a steroid increased fluoroquinolone cytotoxicity.
pubmed.ncbi.nlm.nih.gov/20650258/
Let's start w/ impacts on tenocytes.
A 1996 study found that incubation of human tenocytes w/ ciprofloxacin led to increased cell death.
Addition of a steroid increased fluoroquinolone cytotoxicity.
pubmed.ncbi.nlm.nih.gov/20650258/

9/
Animal models have found edema and increased mononuclear infiltration into the tendons of rats treated with high doses of various fluoroquinolones.
This isn't surprising if tenocyte cytotoxicity is occurring.
pubmed.ncbi.nlm.nih.gov/9371338/
Animal models have found edema and increased mononuclear infiltration into the tendons of rats treated with high doses of various fluoroquinolones.
This isn't surprising if tenocyte cytotoxicity is occurring.
pubmed.ncbi.nlm.nih.gov/9371338/

10/
Under normal circumstances, as we've seen, tenocytes secrete collagen into the ECM, contributing to tendon structure/stability.
Fluoroquinolones impair tenocyte function and survival, which leads to decreased collagen production.
pubmed.ncbi.nlm.nih.gov/10843129/
Under normal circumstances, as we've seen, tenocytes secrete collagen into the ECM, contributing to tendon structure/stability.
Fluoroquinolones impair tenocyte function and survival, which leads to decreased collagen production.
pubmed.ncbi.nlm.nih.gov/10843129/

11/
Next let's examine collagen degradation.
It turns out that fluoroquinolones can upregulate matrix metalloproteinase-2 (MMP-2) activity.
This leads to increased collagen degradation and further weakening of the tendon.
pubmed.ncbi.nlm.nih.gov/20602464/
Next let's examine collagen degradation.
It turns out that fluoroquinolones can upregulate matrix metalloproteinase-2 (MMP-2) activity.
This leads to increased collagen degradation and further weakening of the tendon.
pubmed.ncbi.nlm.nih.gov/20602464/

12/
Tendons constantly undergo a cycle of stress-strain and repair.
In patients w/ other risk factors (eg ESRD, steroid use), fluoroquinolones hamper tendon repair mechanisms, altering this stress-strain relationship and increasing the risk of rupture.
pubmed.ncbi.nlm.nih.gov/18261674/
Tendons constantly undergo a cycle of stress-strain and repair.
In patients w/ other risk factors (eg ESRD, steroid use), fluoroquinolones hamper tendon repair mechanisms, altering this stress-strain relationship and increasing the risk of rupture.
pubmed.ncbi.nlm.nih.gov/18261674/

13/
A convenient way to conceptualize this overall process is that fluoroquinolone tendinopathy is essentially an accelerated form of overuse injury.
A convenient way to conceptualize this overall process is that fluoroquinolone tendinopathy is essentially an accelerated form of overuse injury.
14/
Fluoroquinolones also are associated with an increased of risk of aortic aneurysm and dissection.
This 2019 metanalysis found an overall relative risk elevation for aortopathy of 2.1.
pubmed.ncbi.nlm.nih.gov/30947680/
Fluoroquinolones also are associated with an increased of risk of aortic aneurysm and dissection.
This 2019 metanalysis found an overall relative risk elevation for aortopathy of 2.1.
pubmed.ncbi.nlm.nih.gov/30947680/

15/
The mechanisms for fluoroquinolone-associated aortopathy appears to be similar to tendinopathy.
This mouse study found increased aortic MMP activity and more elastic fiber degradation after ciprofloxacin exposure.
pubmed.ncbi.nlm.nih.gov/30046809/
The mechanisms for fluoroquinolone-associated aortopathy appears to be similar to tendinopathy.
This mouse study found increased aortic MMP activity and more elastic fiber degradation after ciprofloxacin exposure.
pubmed.ncbi.nlm.nih.gov/30046809/

16/SUMMARY
🦶Fluoroquinolones increase the risk of tendinopathy
🦶Mechanisms include tenocyte toxicity, inflammatory responses, ⬇️ collagen production, and ⬆️ collagen degradation
🦶Aortopathy can occur by a similar mechanism
🦶Fluoroquinolones increase the risk of tendinopathy
🦶Mechanisms include tenocyte toxicity, inflammatory responses, ⬇️ collagen production, and ⬆️ collagen degradation
🦶Aortopathy can occur by a similar mechanism
• • •
Missing some Tweet in this thread? You can try to
force a refresh