Veno-occlusive disease (VOD) is one of the worst and a potentially life-threatening complication that can occur after blood or marrow transplantation (BMT).
What is it and how do we manage this?
A 🧵for #MedTwitter trainees in preparation for #EBMT23 ♥️
1/15
What is it and how do we manage this?
A 🧵for #MedTwitter trainees in preparation for #EBMT23 ♥️
1/15
VOD:
-clinical syndrome which can occur after BMTand, less commonly, after chemo, toxic alkaloids, high doses of radiotherapy, or liver transplant
-incidence varies from 2-60% because of different setting, application of different diagnostic criteria and BMT procedures
2/15
-clinical syndrome which can occur after BMTand, less commonly, after chemo, toxic alkaloids, high doses of radiotherapy, or liver transplant
-incidence varies from 2-60% because of different setting, application of different diagnostic criteria and BMT procedures
2/15
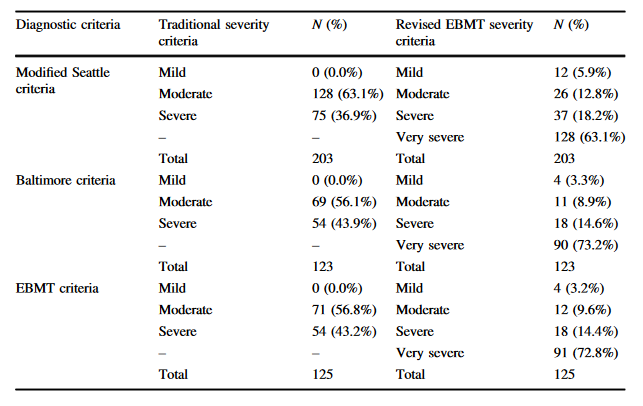
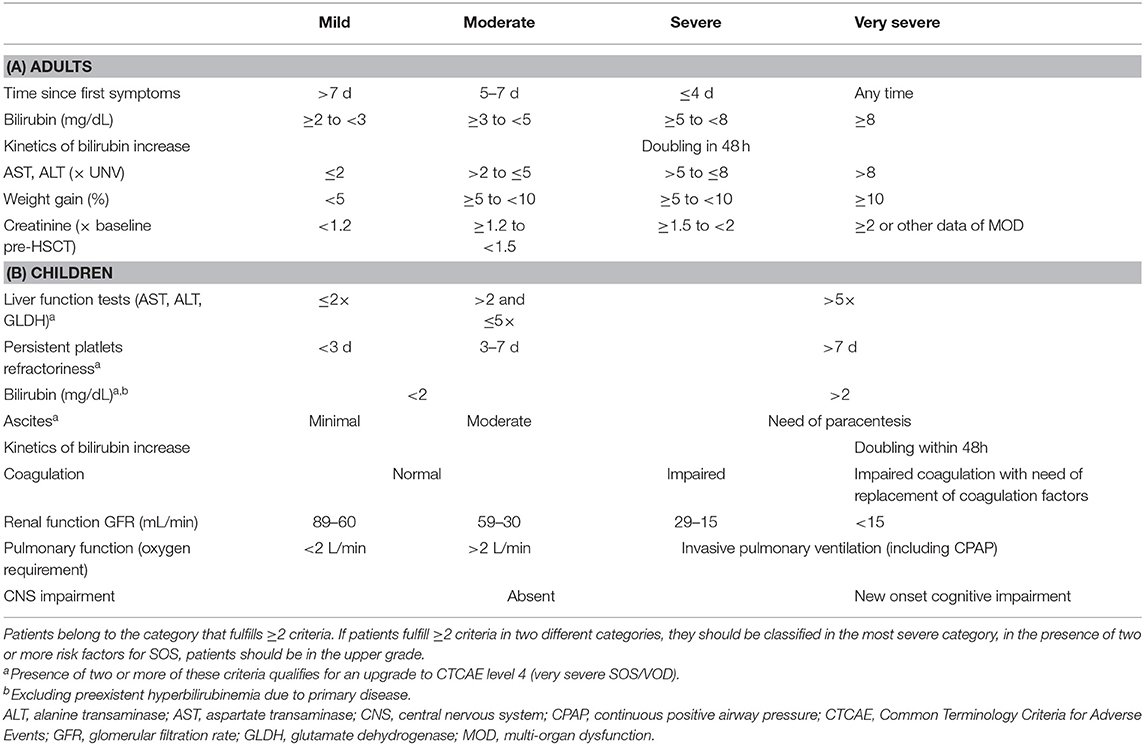
Clinic:
-rapid weight gain, often unresponsive to diuretics, hyperbilirubinemia, painful hepatomegaly, & ascites
-within 21 days after BMT
-late-onset VOD a distinct feature, occurring in 39.3% and 16.7%, respectively, in the adult and pediatric setting
-@TheEBMT criteria👇
3/15
-rapid weight gain, often unresponsive to diuretics, hyperbilirubinemia, painful hepatomegaly, & ascites
-within 21 days after BMT
-late-onset VOD a distinct feature, occurring in 39.3% and 16.7%, respectively, in the adult and pediatric setting
-@TheEBMT criteria👇
3/15
A challenge called VOD!
-high mortality
-multiorgan disease, involving 🫁 + 🫘 function👉dismal outcome
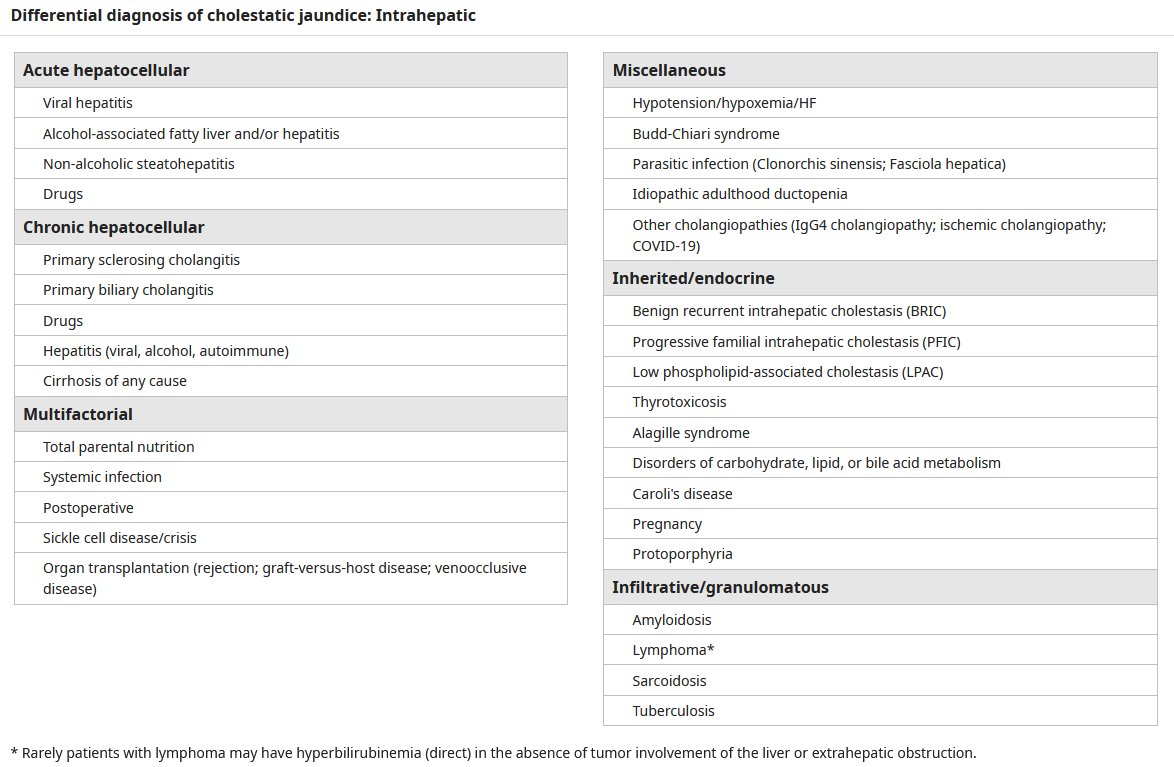
-constrictive pericarditis, different ascites, drug-induced cholestasis and liver injury , sepsis etc make real-life differential diagnosis a true challenge or pitfall
4/15
-high mortality
-multiorgan disease, involving 🫁 + 🫘 function👉dismal outcome
-constrictive pericarditis, different ascites, drug-induced cholestasis and liver injury , sepsis etc make real-life differential diagnosis a true challenge or pitfall
4/15
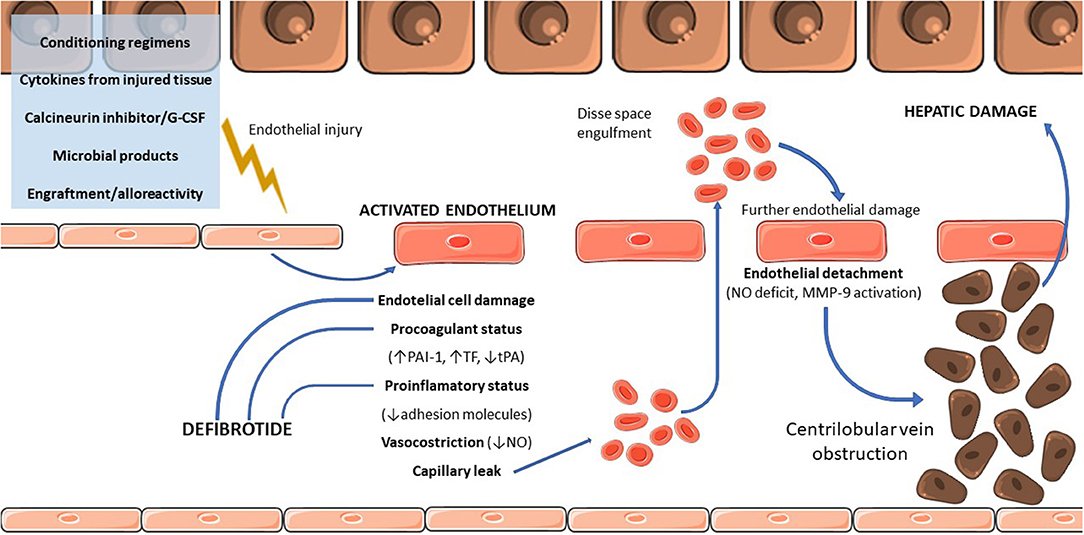
Pathophysiology:
-liver sinusoidal endothelium injury👉loss of cell cohesions👉gaps in endothelial barrier👉RBC pass through👉accumulate in Disse space👉embolization👉postsinusoidal obstruction
-cell detachment~nitric oxide deficiency👉matrix metalloproteinase 9
5/15
-liver sinusoidal endothelium injury👉loss of cell cohesions👉gaps in endothelial barrier👉RBC pass through👉accumulate in Disse space👉embolization👉postsinusoidal obstruction
-cell detachment~nitric oxide deficiency👉matrix metalloproteinase 9
5/15
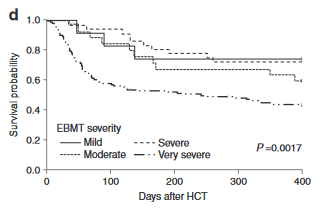
Outcome:
-mortality rates can reach up to 80% in the severe forms
Risk factors:
-liver and lung disease
-preparative regimen for BMT
-graft source
-GVHD prophylaxis (sirolimus, cyclophosphamide, MTX with busulfan)
-monoclonal antibodies conjugated with calicheamicin (GO)
6/15
-mortality rates can reach up to 80% in the severe forms
Risk factors:
-liver and lung disease
-preparative regimen for BMT
-graft source
-GVHD prophylaxis (sirolimus, cyclophosphamide, MTX with busulfan)
-monoclonal antibodies conjugated with calicheamicin (GO)
6/15
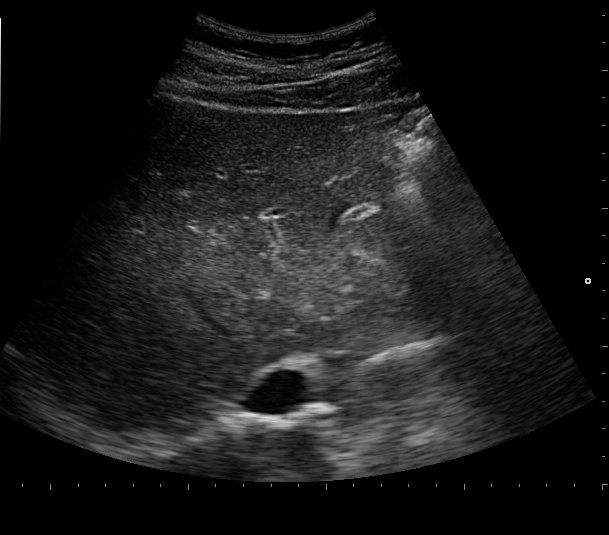
Evaluation:
-clinic and lab work up including hemostasis parameters
-ultrasound!!!👉abnormal portal vein waveform, marked thickening of the gallbladder wall, and a hepatic artery resistance index >0.75
-liver biopsy (transjugular)
7/15
-clinic and lab work up including hemostasis parameters
-ultrasound!!!👉abnormal portal vein waveform, marked thickening of the gallbladder wall, and a hepatic artery resistance index >0.75
-liver biopsy (transjugular)
7/15
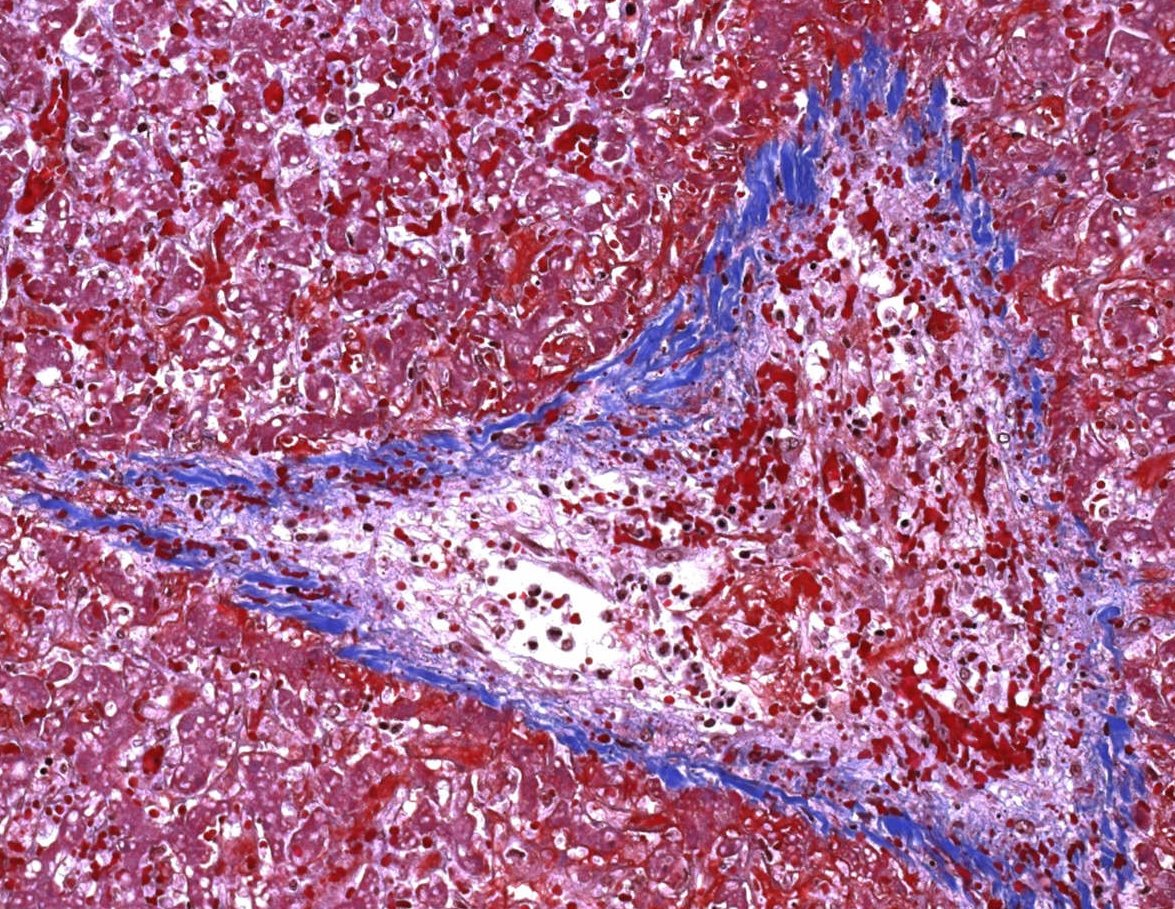
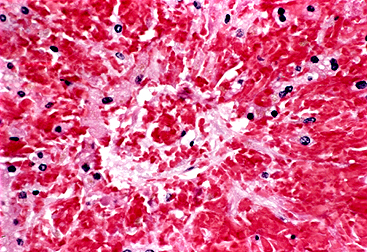
Pathology:
-dilated sinusoids, congested by erythrocytes and nonthrombotic fibrous occlusion of the central veins and small venules
-severe cases: widespread zonal liver disruption and centrilobular hemorrhagic necrosis
-collagen, sclerosis, fibrosis of venular lumens
8/15
-dilated sinusoids, congested by erythrocytes and nonthrombotic fibrous occlusion of the central veins and small venules
-severe cases: widespread zonal liver disruption and centrilobular hemorrhagic necrosis
-collagen, sclerosis, fibrosis of venular lumens
8/15
Treatment:
-by severity
-mild/moderate👉supportive care measures alone but MUST be monitored (maintain euvolumina, avoid hepatotoxic agents, paracentesis)
-severe👉defibrotide
9/15
-by severity
-mild/moderate👉supportive care measures alone but MUST be monitored (maintain euvolumina, avoid hepatotoxic agents, paracentesis)
-severe👉defibrotide
9/15

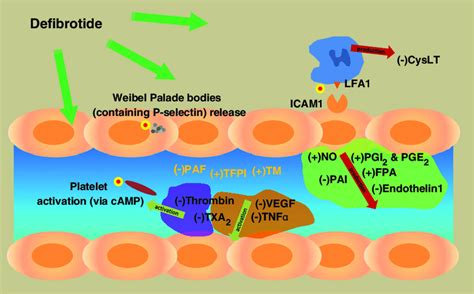
Defibrotide:
-sodium salt of single-stranded oligodeoxyribonucleotides derived from DNA of porcine intestinal mucosa
-mechanism unclear
-inhibit the activation of endothelial cells, reduce inflammation and oxidative stress, and enhance the production of nitric oxide
10/15
-sodium salt of single-stranded oligodeoxyribonucleotides derived from DNA of porcine intestinal mucosa
-mechanism unclear
-inhibit the activation of endothelial cells, reduce inflammation and oxidative stress, and enhance the production of nitric oxide
10/15
Defibrotide administration:
-6.25 mg/kg every 6 hours IV for ≥21 days, until resolution or hospital discharge, maximum of 60 days
-discontinue ≥2 hours prior to invasive procedures and can be resumed
-check Hb/platelets frequently during treatment (PLT target best >30k)
11/15
-6.25 mg/kg every 6 hours IV for ≥21 days, until resolution or hospital discharge, maximum of 60 days
-discontinue ≥2 hours prior to invasive procedures and can be resumed
-check Hb/platelets frequently during treatment (PLT target best >30k)
11/15

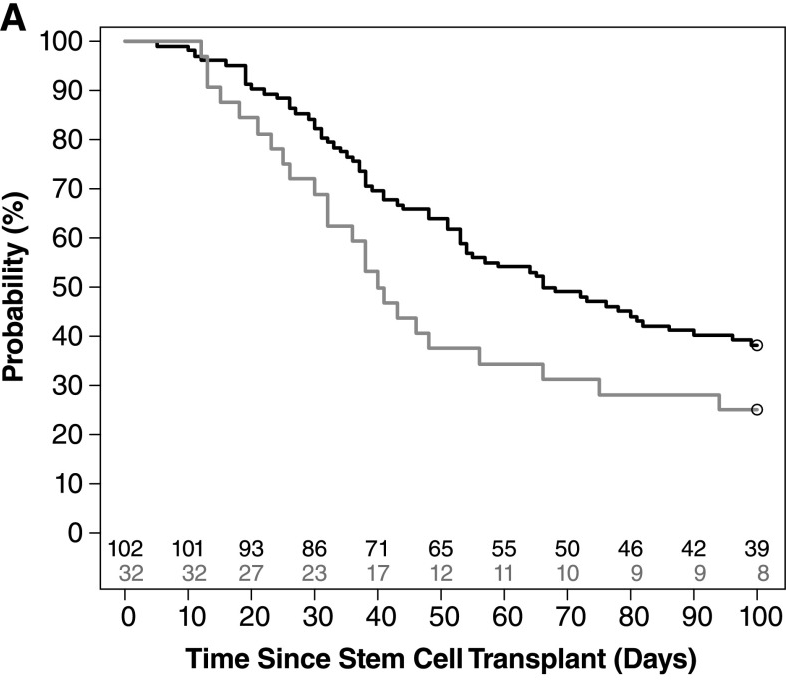
Defibrotide outcome:
-multicenter study of children and adults compared with 32 historical control patients👉defibrotide with superior day +100 survival (38 versus 25%) and day +100
-fatal hemorrhagic events were reported in 15% of defibrotide versus 6% of controls
12/15
-multicenter study of children and adults compared with 32 historical control patients👉defibrotide with superior day +100 survival (38 versus 25%) and day +100
-fatal hemorrhagic events were reported in 15% of defibrotide versus 6% of controls
12/15
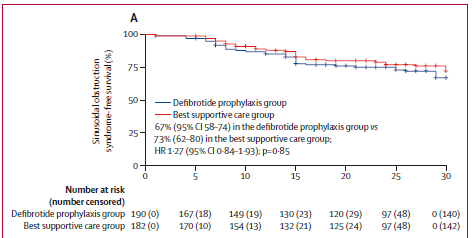
Prophylaxis:
-for adults, ursodeoxycholic acid can be considered from conditioning rather than no prophylaxis👉naturally-occurring hydrophilic bile acid👉reducing hydrophobicity of other naturally-occurring bile acids
-NOT defibrotide, as shown again recently @TheLancetHaem
13/15
-for adults, ursodeoxycholic acid can be considered from conditioning rather than no prophylaxis👉naturally-occurring hydrophilic bile acid👉reducing hydrophobicity of other naturally-occurring bile acids
-NOT defibrotide, as shown again recently @TheLancetHaem
13/15
Refractory VOD:
No pharmacologic agent has proven benefit for patients with severe hepatic SOS who do not respond adequately to ≥3 weeks of defibrotide treatment.
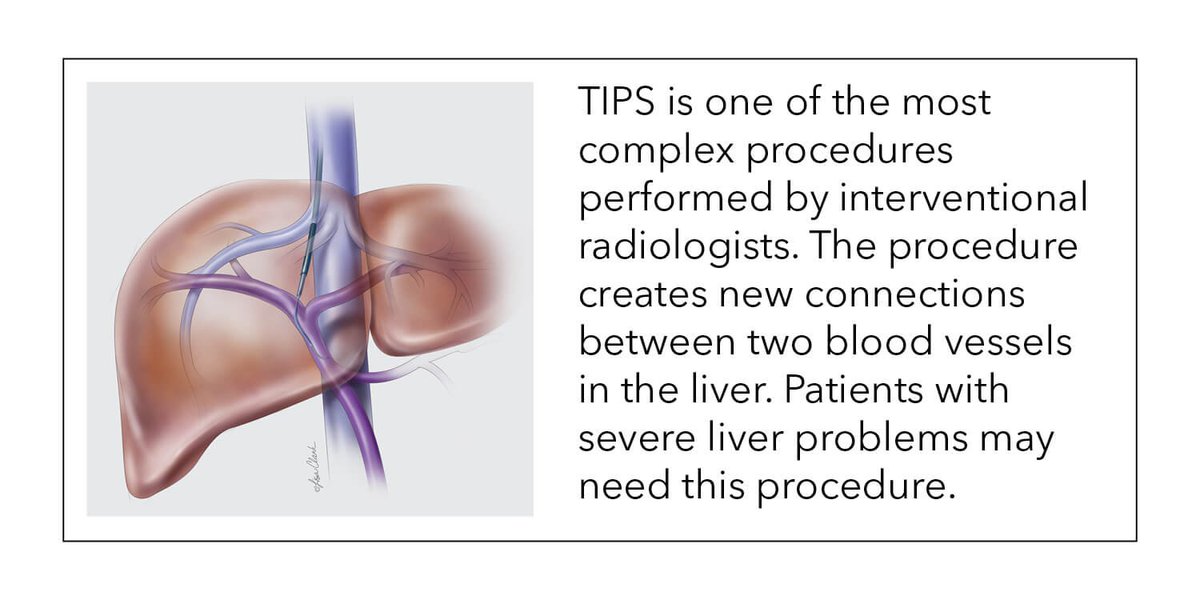
Consider:
-TIPS (also in acute disease)
-methylprednisolone
-liver transplant
14/15
No pharmacologic agent has proven benefit for patients with severe hepatic SOS who do not respond adequately to ≥3 weeks of defibrotide treatment.
Consider:
-TIPS (also in acute disease)
-methylprednisolone
-liver transplant
14/15
Summary of VOD:
❗️life-threatening, high mortality
❗️~15% of adults after BMT
❗️careful monitoring required to make diagnosis
❗️prompt treatment needed
❗️supportive care for mild/moderate
❗️defibrotide for severe
❗️TIPS for acute or refractory disease
❗️UDCA only prophylaxis
Fin.
❗️life-threatening, high mortality
❗️~15% of adults after BMT
❗️careful monitoring required to make diagnosis
❗️prompt treatment needed
❗️supportive care for mild/moderate
❗️defibrotide for severe
❗️TIPS for acute or refractory disease
❗️UDCA only prophylaxis
Fin.
Sources and references:
ashpublications.org/bloodadvances/…
frontiersin.org/articles/10.33…
nature.com/articles/s4140…
humpath.com/spip.php?artic…
ashpublications.org/bloodadvances/…
frontiersin.org/articles/10.33…
nature.com/articles/s4140…
humpath.com/spip.php?artic…
• • •
Missing some Tweet in this thread? You can try to
force a refresh