1/Talk about the bases being loaded!
Central skull base has some of the most complicated anatomy & pathology in neuro
Do you know how to approach it?
Here’s a #tweetorial to show you how diagnose lesions at the central skullbase!
#meded #medtwitter #FOAMed #neurosurgery
Central skull base has some of the most complicated anatomy & pathology in neuro
Do you know how to approach it?
Here’s a #tweetorial to show you how diagnose lesions at the central skullbase!
#meded #medtwitter #FOAMed #neurosurgery

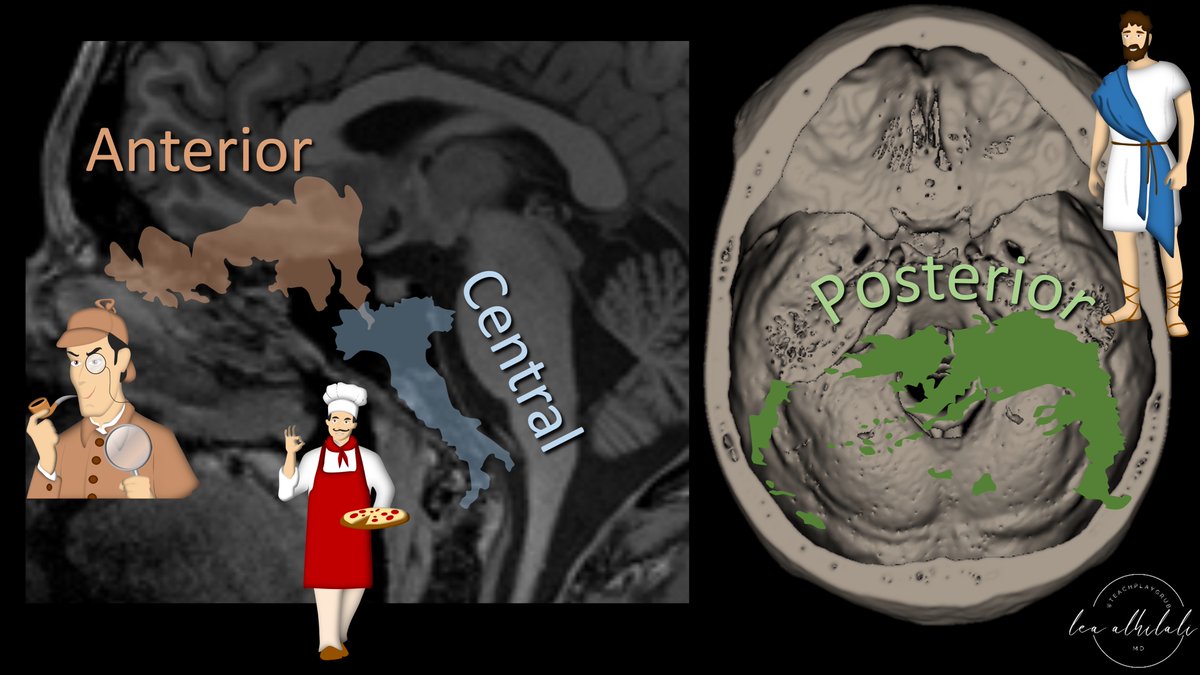
2/Think of the skullbase divisions like different countries—each w/their own culture. Each division has lesions that are specific to it—just like countries have food that are specific to them.
I think the central skullbase looks like Italy, hanging down from the ant. skullbase
I think the central skullbase looks like Italy, hanging down from the ant. skullbase

3/Lesions can involve the central skullbase from below, within, or above
Let’s start from below. Nasopharynx is below the central skullbase. Nasopharyngeal carcinomas (NPC) can invade from below
Using our Italy theme, you can remember this bc NPC look like an Italian meatball
Let’s start from below. Nasopharynx is below the central skullbase. Nasopharyngeal carcinomas (NPC) can invade from below
Using our Italy theme, you can remember this bc NPC look like an Italian meatball

4/Central skullbase can also be involved from below by perineural tumor spread, as it is the home of the cranial nerves.
You can remember this w/our Italy theme bc the tumor spreads along the twisty nerves like Italian pasta
You can remember this w/our Italy theme bc the tumor spreads along the twisty nerves like Italian pasta

5/One unique lesion to involve the central skullbase from below is the juvenile angiofibroma. This occurs in teenage boys & is centered at the sphenopalatine foramen. It’s very vascular & commonly causes w/epistaxis
You can remember this bloody tumor bc Italian sauces are RED
You can remember this bloody tumor bc Italian sauces are RED

6/Now let’s look at lesions from within. Lesions arising from the marrow are common in the central skullbase bc it has abundant marrow. Most commonly, it’s metastases & myeloma. You can remember marrow lesions are common here, bc bone marrow is an Italian delicacy

7/Unique lesions to the central skullbase that arise from within are notochordal from the notochordal remnants that live in this region.
Using our Italian theme, you can remember this bc Noto is a city in Sicily—we actually vacationed there last year!
Using our Italian theme, you can remember this bc Noto is a city in Sicily—we actually vacationed there last year!

8/Notochordal lesions are spectrum, ranging from the most aggressive, chordoma, to the more benign ecchordosis physaliphora & benign notochordal cell tumors.
How do you tell these lesions apart from each other & from other skullbase lesions?
How do you tell these lesions apart from each other & from other skullbase lesions?

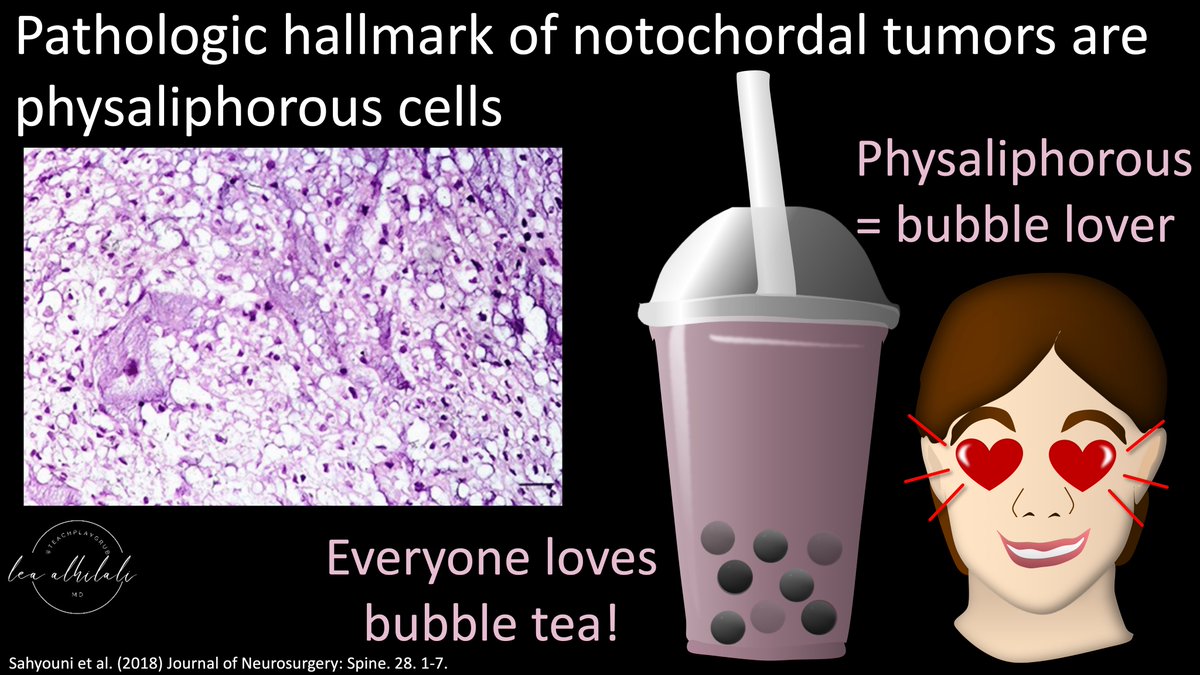
9/Pathologic hallmark of notochordal cell tumors is physaliphorous cells. Physaliphorous means bubble lover, because the cells look like big empty bubbles.
This makes me think of bubble tea. Unfortunately, bubble tea isn’t Italian to help you remember this, but it is delicious!
This makes me think of bubble tea. Unfortunately, bubble tea isn’t Italian to help you remember this, but it is delicious!
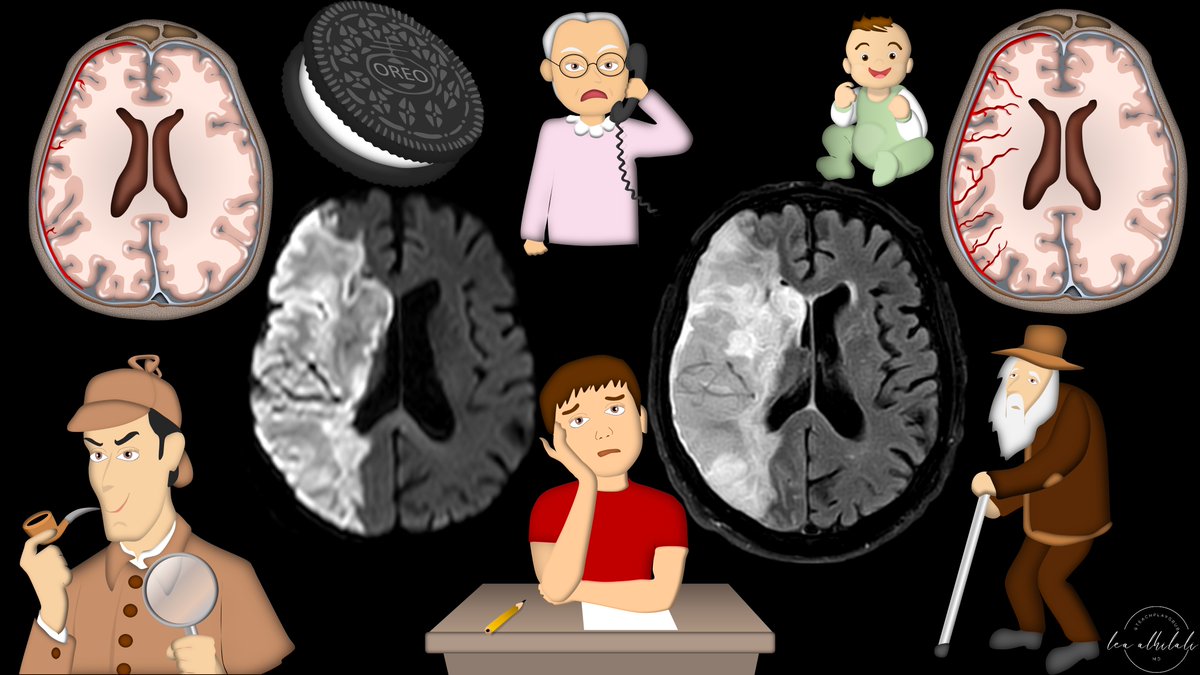
10/You can think of these bubble cells like water balloons—they are filled with fluid.
So what does a lot of water mean? Bright on T2!
These lesions are super bright on T2 bc they have these water filled cells.
So what does a lot of water mean? Bright on T2!
These lesions are super bright on T2 bc they have these water filled cells.

11/Most common notochordal lesions are chordoma & ecchordosis. They are actually like twins that were separated at birth.
They look identical to pathologists but they have very different behaviors. In fact, ecchordosis used be called “intradural chordoma.”
They look identical to pathologists but they have very different behaviors. In fact, ecchordosis used be called “intradural chordoma.”

12/It’s like they were twins separated at birth & raised differently.
Chordoma was raised extradurally, on the wrong side of the tracks, on the rough side of town, away from the safe intradural space—while ecchordosis was coddled by the warm protection of the dura
Chordoma was raised extradurally, on the wrong side of the tracks, on the rough side of town, away from the safe intradural space—while ecchordosis was coddled by the warm protection of the dura

13/Bc chordoma was raised on the wrong side of the dura, it is more like to, well, light up—or enhance on imaging.
Whereas the properly raised ecchordosis is unlikely to find a pipe & light up, so it rarely enhances
Whereas the properly raised ecchordosis is unlikely to find a pipe & light up, so it rarely enhances

14/Another finding that can help you differentiate is a bony spur. A bony spur is pathognomonic for ecchordosis.
I remember this bc only a lesion raised in the comfort of the intradural space, very privileged, can afford a Bentley Spur
I remember this bc only a lesion raised in the comfort of the intradural space, very privileged, can afford a Bentley Spur

15/In between ecchordosis & chordoma is the benign notochordal cell tumor (BNCT).
It’s like their cousin, who was raised on the wrong side of the tracks (extra-dural) but was somehow able to turn their life around—so they don’t light up
BNCT are extradural but do not enhance
It’s like their cousin, who was raised on the wrong side of the tracks (extra-dural) but was somehow able to turn their life around—so they don’t light up
BNCT are extradural but do not enhance

16/BNCT is like a kid who made it out the hood growing up extradural to be a success & not light up.
But bc it had a tough time growing up, it was scarred or sclerosed by the experience. So BNCT have sclerosis on CT
But bc it had a tough time growing up, it was scarred or sclerosed by the experience. So BNCT have sclerosis on CT
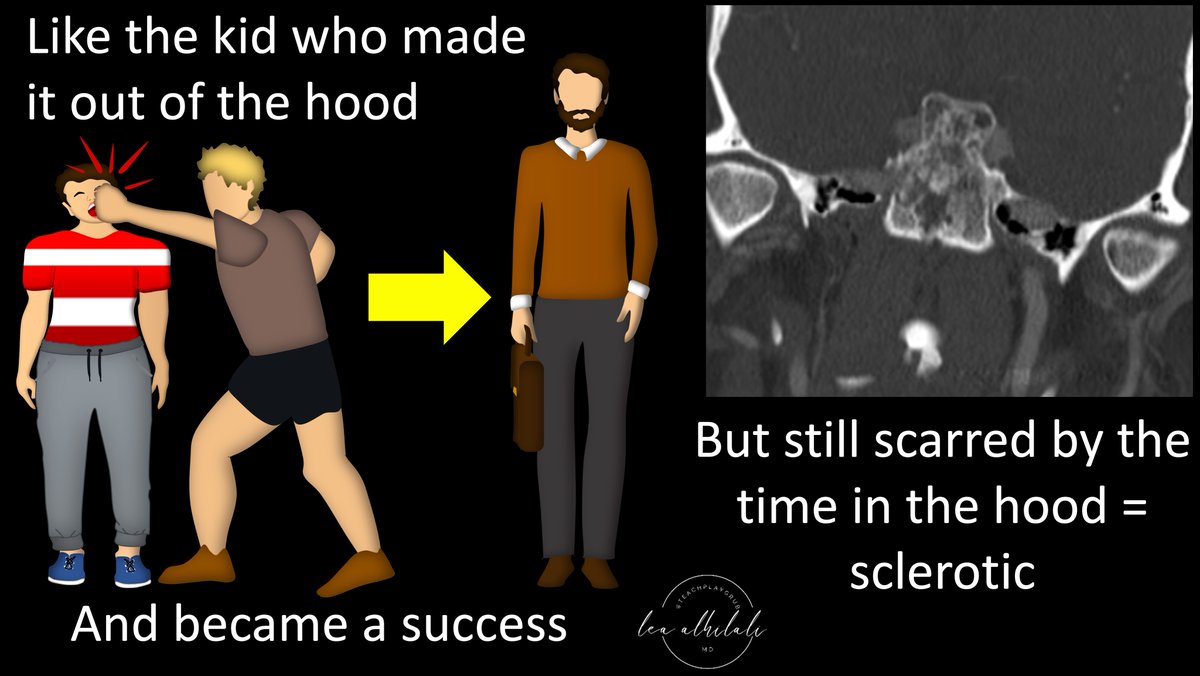
17/Because of the sclerosis, BNCT can mimic fibrous dysplasia on CT, with mixed lytic & sclerotic findings.
But bc they are a notochordal cell tumor, they are bright on T2 from the physaliphorous cells, unlike fibrous dyplasia which is T2 dark from its fibrous component.
But bc they are a notochordal cell tumor, they are bright on T2 from the physaliphorous cells, unlike fibrous dyplasia which is T2 dark from its fibrous component.

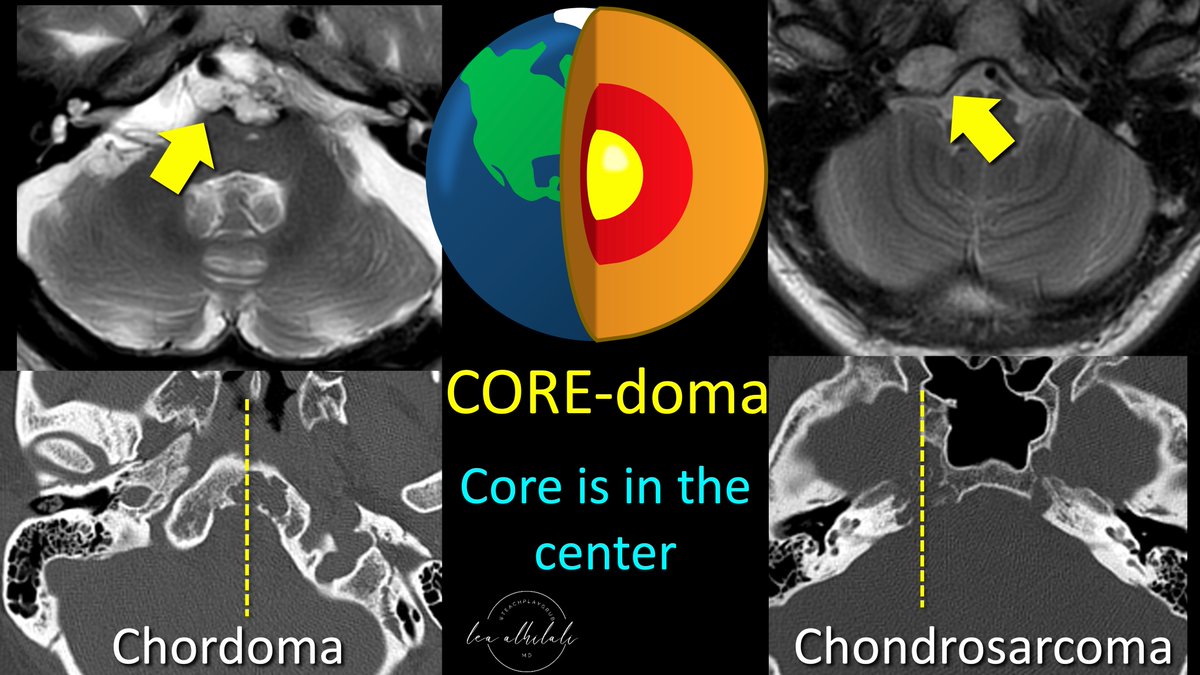
18/Another T2 bright central skullbase lesion is chondrosarcoma. It’s aggressive & can mimic a chordoma on MRI.
You can differentiate them by their position. Chordoma is midline, while chondrosarcoma is off midline.
I remember this bc CORE-doma is central or in the core
You can differentiate them by their position. Chordoma is midline, while chondrosarcoma is off midline.
I remember this bc CORE-doma is central or in the core
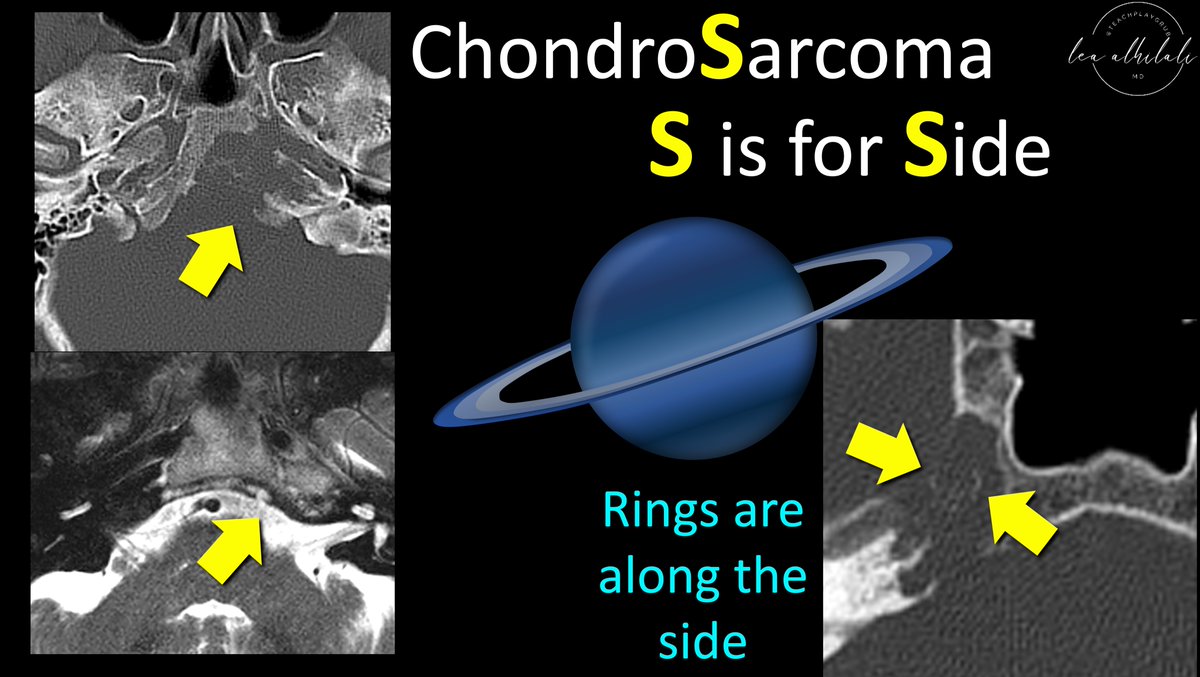
19/I remember chondrosarcoma is off midline bc it’s a Sarcoma & Sarcoma and Side both start w/S.
On CT, you can see rings & arcs matrix. This makes sense bc rings aren’t in the CORE of a planet, they’re along the SIDE.
On CT, you can see rings & arcs matrix. This makes sense bc rings aren’t in the CORE of a planet, they’re along the SIDE.
20/Finally, lesions from above.
At the central skull base, these are overwhelming aggressive pituitary adenomas.
Using our Italian theme, I remember this bc pituitary sounds like an Italian insult they might hurl at you with some classic hand gestures😉
At the central skull base, these are overwhelming aggressive pituitary adenomas.
Using our Italian theme, I remember this bc pituitary sounds like an Italian insult they might hurl at you with some classic hand gestures😉

21/So now you can use our Italian theme to remember the most common central skullbase lesions that involve this region from below, within, or above.
Please stay tuned for more BASICS of skullBASE as next I will tackle the posterior skullbase. Alla prossima!
Please stay tuned for more BASICS of skullBASE as next I will tackle the posterior skullbase. Alla prossima!
• • •
Missing some Tweet in this thread? You can try to
force a refresh