What is the most likely diagnosis in this 30 y/o w/ history of discitis/osteomyelitis presenting w/ fevers, chills, and neck pain? 🧠
#ent #Neurosurgery #Neurology #medtwitter #MedEd @The_ASSR #NeuroTwitter
#ent #Neurosurgery #Neurology #medtwitter #MedEd @The_ASSR #NeuroTwitter




Answer: Longus Colli Calcific Tendinitis
▶️Etiology: inflammatory reaction in response to deposition of calcium hydroxyapatite crystals (just like in the rotator cuff)
▶️This case is a bit tricky as the history is somewhat misleading (though it often is in radiology)
▶️Etiology: inflammatory reaction in response to deposition of calcium hydroxyapatite crystals (just like in the rotator cuff)
▶️This case is a bit tricky as the history is somewhat misleading (though it often is in radiology)
Imaging:
▶️Sagittal STIR shows marked retropharyngeal/prevertebral edema (yellow arrow) and focal hypointensity from the hydroxyapatite crystals (green arrow)
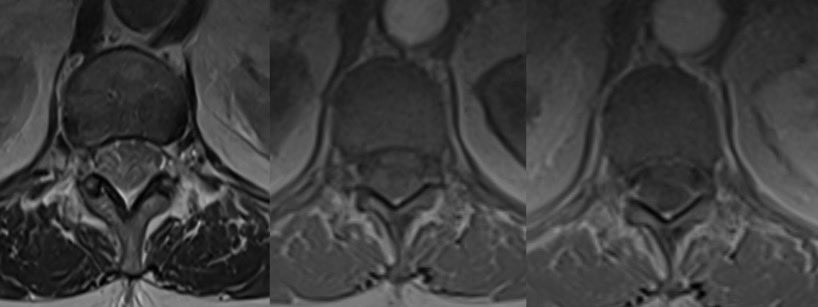
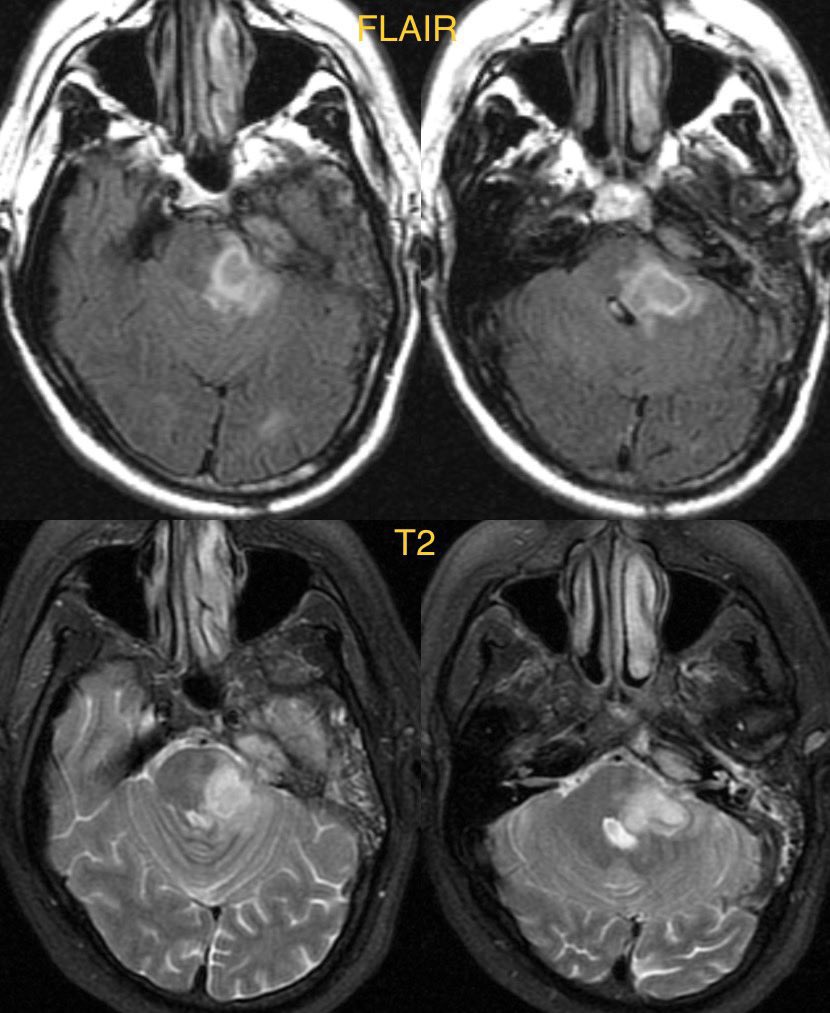
▶️Axial T2 again shows the marked edema
▶️Sagittal STIR shows marked retropharyngeal/prevertebral edema (yellow arrow) and focal hypointensity from the hydroxyapatite crystals (green arrow)
▶️Axial T2 again shows the marked edema


▶️T2* is key in this case showing the markedly hypointense amorphous calcs at the longus colli tendons
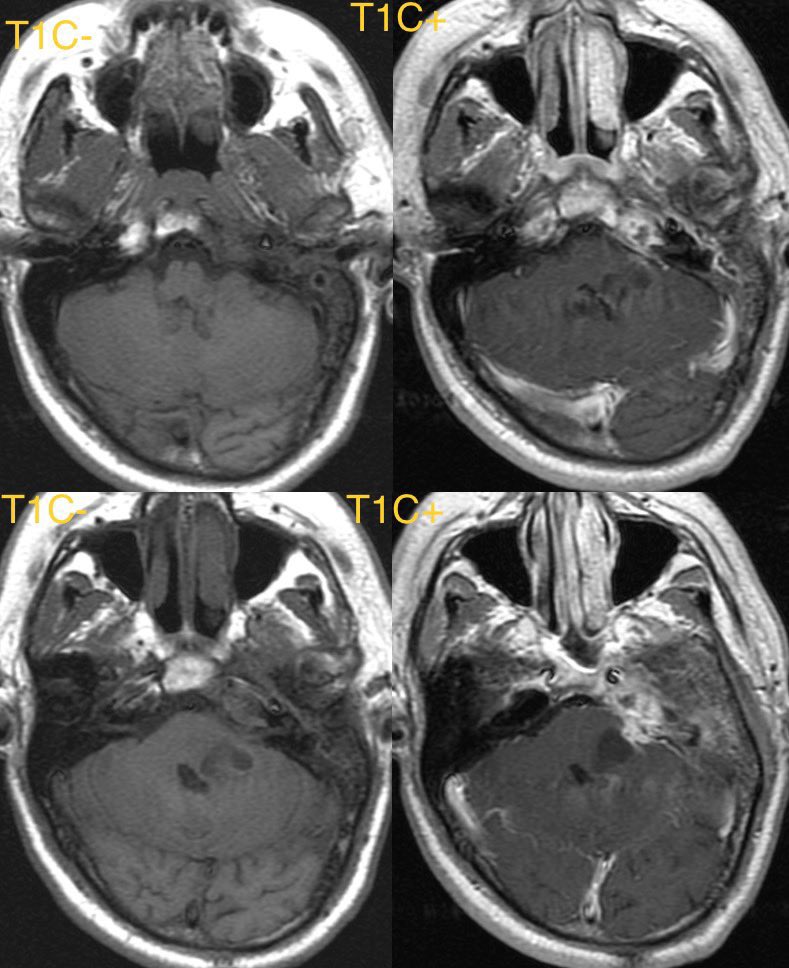
▶️Pre and post con T1 shows the edema w/ reactive enhancement (yellow arrows) and the focal hypointense calcs (green arrows)
▶️Pre and post con T1 shows the edema w/ reactive enhancement (yellow arrows) and the focal hypointense calcs (green arrows)


General imaging features:
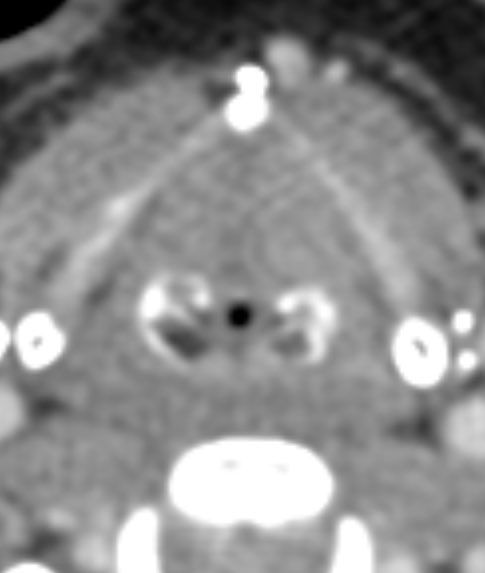
▶️Amorphous calcifications at C1-C2 junction near the insertion of the longus colli muscles is pathognomonic
▶️ Be careful not to mix up calcification at the C1-C2 junction w/ the more common COARSE calcs in DJD!
▶️Amorphous calcifications at C1-C2 junction near the insertion of the longus colli muscles is pathognomonic
▶️ Be careful not to mix up calcification at the C1-C2 junction w/ the more common COARSE calcs in DJD!
Imaging cont:
▶️Calcs on MR can be trickier, look for MARKED FOCAL HYPOINTENSITY on T2*/GRE at the C1-C2 JUNCTION
▶️Expect prevertebral and/or retropharyngeal edema
▶️Reactive soft tissue enhancement on T1C+
▶️Calcs on MR can be trickier, look for MARKED FOCAL HYPOINTENSITY on T2*/GRE at the C1-C2 JUNCTION
▶️Expect prevertebral and/or retropharyngeal edema
▶️Reactive soft tissue enhancement on T1C+
DDX:
Must differentiate from infection (as calcific tendinitis is treated with time and NSAIDs)
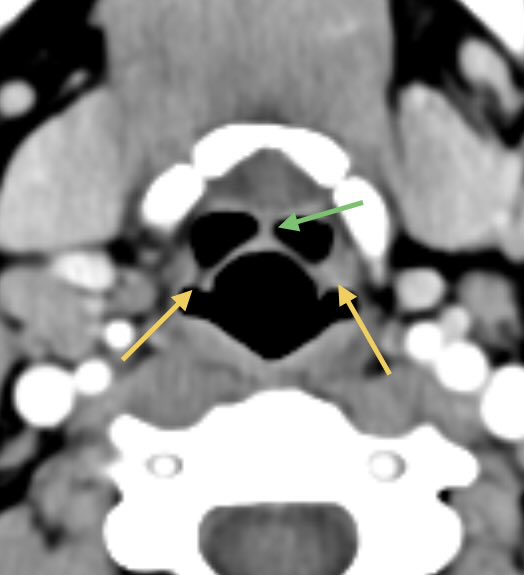
▶️For infection, expect a more spherical or convex retropharyngeal collection, more enhancement, and presence of head and neck infection
Must differentiate from infection (as calcific tendinitis is treated with time and NSAIDs)
▶️For infection, expect a more spherical or convex retropharyngeal collection, more enhancement, and presence of head and neck infection
▶️Calcifications at the C1-C2 junction are pathognomonic for calcific longus colli tendonitis 🧠
Companion cases:
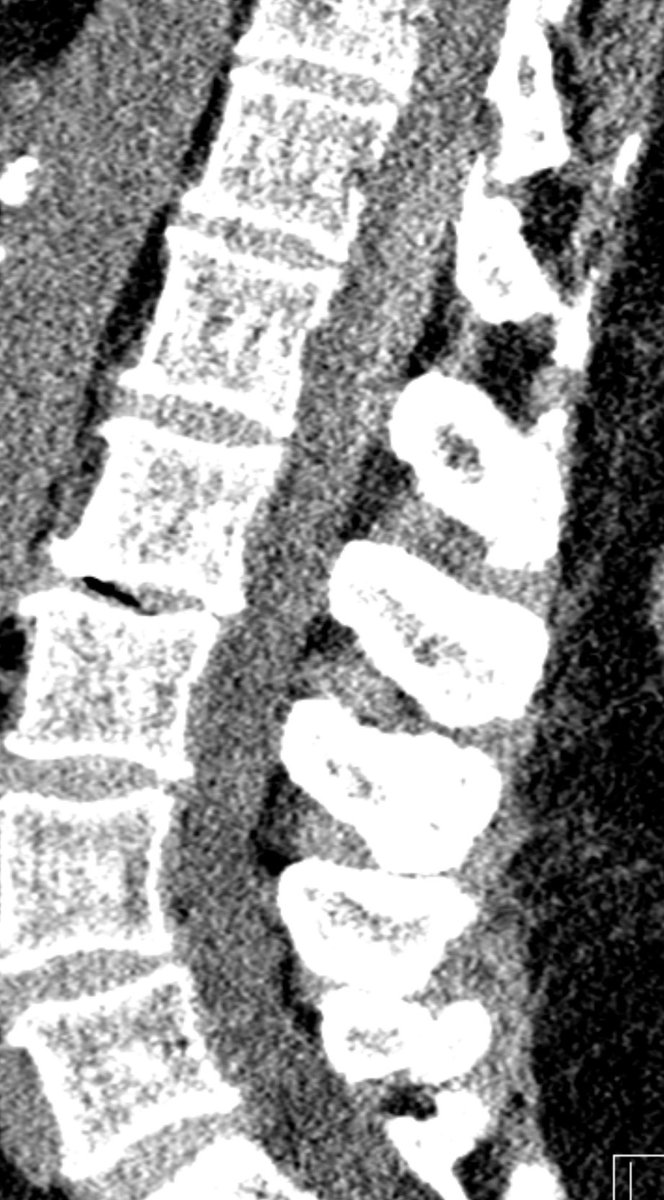
▶️Radiograph showing prevertebral swelling and amorphous calcs on C1-C2 junction
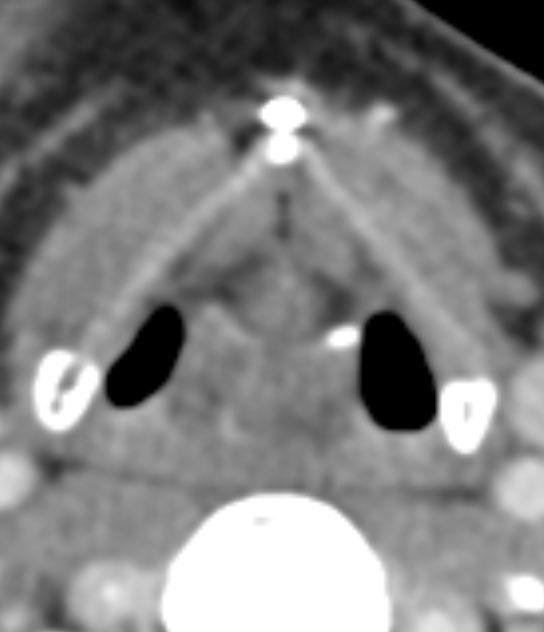
▶️Appearance on CT in a different patient showing the amorphous calcs and edema
Companion cases:
▶️Radiograph showing prevertebral swelling and amorphous calcs on C1-C2 junction
▶️Appearance on CT in a different patient showing the amorphous calcs and edema



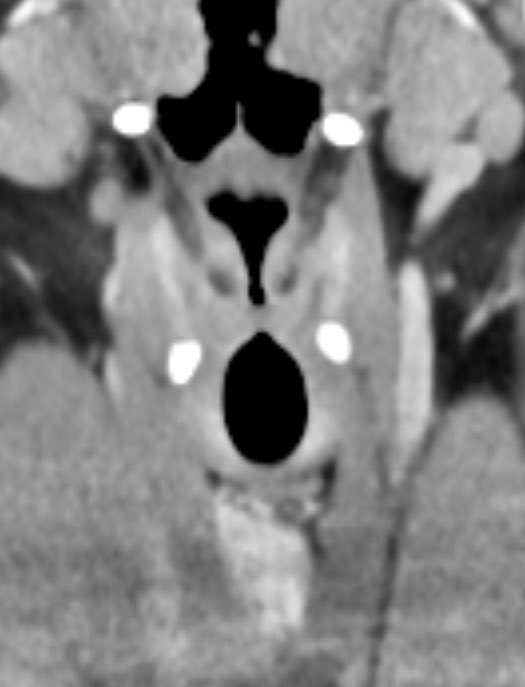
Companion case 3 (DJD fake out!!):
▶️CT shows COARSE calcifications at C1-C2 junction with mild pharyngeal edema (from prior radiation in this case)
▶️CT shows COARSE calcifications at C1-C2 junction with mild pharyngeal edema (from prior radiation in this case)


• • •
Missing some Tweet in this thread? You can try to
force a refresh