🇺🇸 Yesterday, the FDA approved an RSV vaccine for use in pregnancy.
There was a non-significant difference in preterm birth in the trial, which patients will be informed about.
Let's look at the minutes of the meeting to understand these decisions... 🧵
fda.gov/news-events/pr…
There was a non-significant difference in preterm birth in the trial, which patients will be informed about.
Let's look at the minutes of the meeting to understand these decisions... 🧵
fda.gov/news-events/pr…
Before we start, here are links to the trial report...
And the meeting minutes... 2/
nejm.org/doi/10.1056/NE…
fda.gov/media/169361/d…
And the meeting minutes... 2/
nejm.org/doi/10.1056/NE…
fda.gov/media/169361/d…
RSV is the leading cause of death in babies <6 mo, and is implicated in 50% of hospitalisations for respiratory illness, so development of a vaccine is a priority.
I should declare an interest here... my baby son was very sick with RSV 😢 and I would have loved to avoid that. 3/
I should declare an interest here... my baby son was very sick with RSV 😢 and I would have loved to avoid that. 3/
In the trial, the effectiveness of the vaccine against severe RSV disease in babies under 3 months was 81.8%, meeting one of two pre-specified efficacy goals.
They did not meet the efficacy goal for non-severe disease. 4/
nejm.org/doi/10.1056/NE…

They did not meet the efficacy goal for non-severe disease. 4/
nejm.org/doi/10.1056/NE…

Great! And the committee voted unanimously that efficacy was sufficient to approve this vaccine. 5/
fda.gov/media/169361/d…
fda.gov/media/169361/d…

But what about safety?
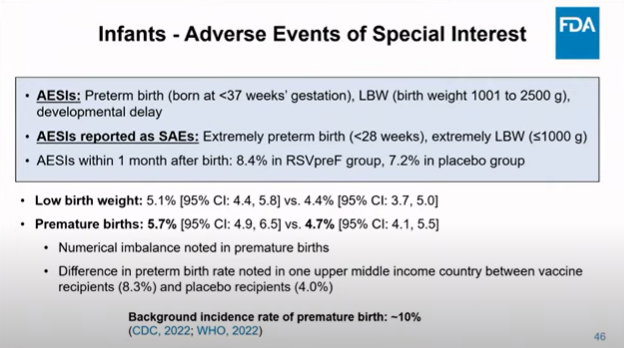
There was no significant difference in any safety outcome, but the committee did spend a long time discussing whether a non-significant difference in preterm birth (4.7% vs 5.7%) was a concern. 6/
nejm.org/doi/10.1056/NE…
There was no significant difference in any safety outcome, but the committee did spend a long time discussing whether a non-significant difference in preterm birth (4.7% vs 5.7%) was a concern. 6/
nejm.org/doi/10.1056/NE…

Looking at the data in more detail, in high and low income countries there was no difference at all in preterm birth rates.
The difference is driven specifically by South Africa. 7/
fda.gov/media/169361/d…
The difference is driven specifically by South Africa. 7/
fda.gov/media/169361/d…
This might give us some reassurance that the difference is due to chance (in line with it not being significant) since it doesn't appear in other countries.
Or it might be a real difference, specific to S. Africa (although this might still be reassuring, for non-SAffers...) 8/
Or it might be a real difference, specific to S. Africa (although this might still be reassuring, for non-SAffers...) 8/
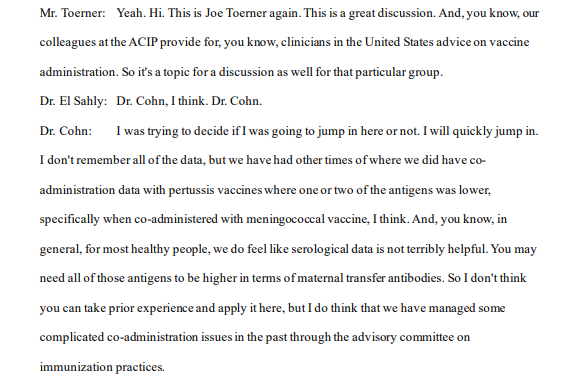
If it is a real effect, a possibility we should consider is that, given this occurs in a massive COVID wave, and that we know COVID can cause preterm birth, the RSV vaccine is interfering with the COVID vaccine. There wasn't the data to address this, though. 9/

But it does feed into wider questions about the possibility that antenatal vaccinations may not work so well if they are co-administered. So, if the RSV vaccine is to be offered, we have to give some consideration to when exactly. 10/
Regardless, the Committee agreed that if they approved the vaccine, it would be important to have a very solid surveillance plan. It was pointed out that a rapid analysis of the Vaccine Safety Data Link could provide firm answers on this in a matter of months. 11/
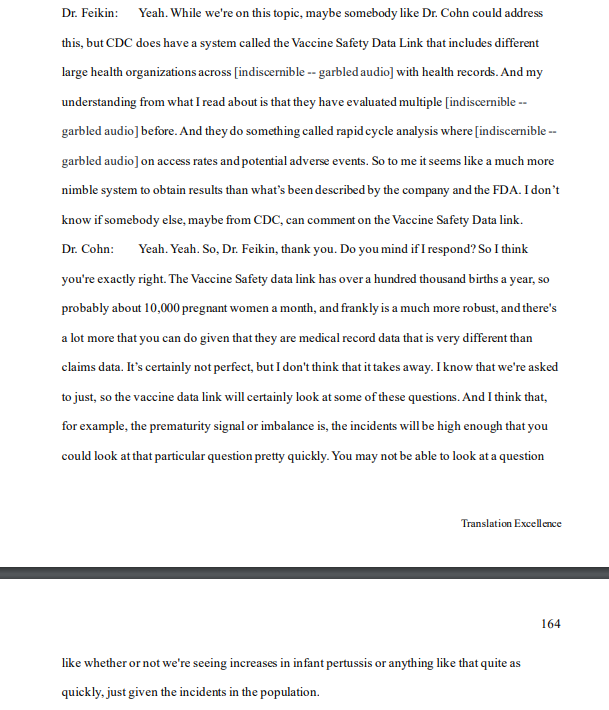
But while this uncertainty persists, of course it's important that people can make a fully informed decision about whether or not they will get vaccinated. So information about this will appear in the documents clinicians use to counsel their patients (the "label"). 12/

After this discussion, the Committee voted on whether to approve the vaccine on the basis of safety. 10 voted for and 4 against. 13/
The final recommendation was to approve the vaccine...
👉🏻 With robust monitoring
👉🏻 Counselling patients about the non-significant difference in preterm birth
👉🏻 Between 32 and 36 weeks, to reduce the risk of preterm birth
14/
fda.gov/news-events/pr…
👉🏻 With robust monitoring
👉🏻 Counselling patients about the non-significant difference in preterm birth
👉🏻 Between 32 and 36 weeks, to reduce the risk of preterm birth
14/
fda.gov/news-events/pr…

Here ends my summary of the meeting minutes, although I would encourage anyone who is interested to read them themselves.
Here also ends my lunchbreak. I will continue this thread with my own views on the decision later today...
15/ (to be continued...)
Here also ends my lunchbreak. I will continue this thread with my own views on the decision later today...
15/ (to be continued...)
• • •
Missing some Tweet in this thread? You can try to
force a refresh