Renal/GIM consultant. Dad. Runner. Poker player. POCUS. #NSMC Intern 2021. @BukuRenal. Associate editor @NephJC.
May 19, 2023 • 20 tweets • 9 min read
1/20
Difelikefalin approved by NICE for uraemic itch in patients on haemodialysis! nice.org.uk/guidance/ta890
(on the same day I was offered a consultant job with a haemodialysis role - also exciting!)
Thread to learn everything you need to know about difelikefalin🧵👇 2/ Quick recap on uraemic itch that will surprise no one:
✳️ Common
✳️ Under-estimated by nephrologists
✳️ Many patients don’t report it unless you ask specifically
✳️ Associates with depression, poor sleep & reduced QoL
✳️ Patients state it’s a priority for research
Apr 22, 2022 • 20 tweets • 6 min read
You get called to the haemodialysis unit.
An 18 yr old man has missed his dialysis all week & today reports weak legs. The dialysis nurse snaps this ECG as he passes out.
What do you do? Is starting dialysis during CPR ever a thing?
A thread on hyperkalaemic cardiac arrest👇 1/ As you can imagine the evidence base for optimal management of hyperkalaemic cardiac arrest is fairly low quality.
Here’s some ideas (majority of which are based on fantastic UKKA 2020 review & algorithm👇), but every tweet comes with the “but no one knows for sure” caveat….
Dec 3, 2021 • 20 tweets • 8 min read
1/ Nephrology:
“We will forever argue about validity of equations to convert serum creatinine to eGFR using age, sex etc”
Also nephrology:
“We will make no adjustment for muscle mass when using urinary creatinine within urine ACR”
A #tweetorial on two albuminuria paradoxes 👇 2/ Recap: why use early morning urine ACR?
✅Correlates well with ‘gold standard’ 24hr urine collection (pain to perform)
✅Creatinine in denominator corrects for urine dilution - works when creat excretion constant (but, note some daily variation)
✅ Many potential factors;
✔️hypovolaemia due to fever / GI symptoms
✔️sepsis & cytokine release
✔️rhabdo, even without myalgia; check CK!
✔️direct viral tubule invasion?
✅ Low grade proteinuria & haematuria common
✅ Don’t miss ‘usual’ post-renal AKI; bladder scan +- US
Mar 1, 2020 • 18 tweets • 6 min read
1/ #medtwitter is fairly comfortable managing “normal” DKA right? But how about in the anuric dialysis patient? The cookbook protocol can be deadly.
Read this #tweetorial to learn about how their DKA pathophysiology is fascinatingly different.
✅ “stress hormones” rise
✅ blood glucose rises & because glucose is an osmotic diuretic, there is a huge, inappropriate urine output
✅ body makes ketones as alternative fuel, so pH falls
Jan 26, 2020 • 14 tweets • 7 min read
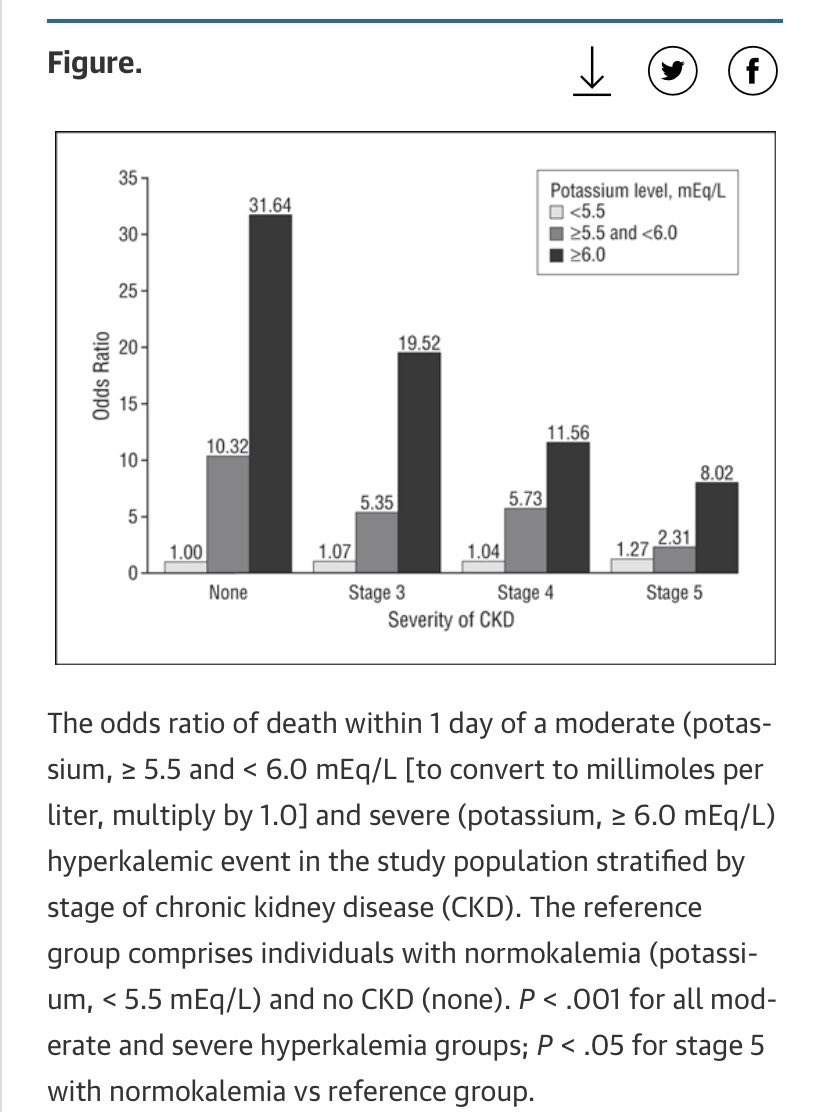
1/ Hyperkalaemia treatment
KDIGO have just published their conference conclusions on managing acute #hyperkalaemia so I run through some learning points, some criticisms and the bits I’m not sure about as a renal reg.
Last week twitter was unexpectedly keen for renal registrar on-call tips, so here’s round 2️⃣ of kidney #tipsfornewdocs covering iv fluids, AKI, “renal screen” bloods, immunosuppression, electrolytes, DKA in ESKD, peritoneal dialysis, proteinuria, meds & ⬆️BP (thread) #nephpearls
Iv fluids; Renal #tipsfornewdocs 2️⃣ 1/15
✅ 1L 5% dextrose 12 hourly = 50g glucose = 55 skittles. Not same as feeding patient.
✅ “iv fluid for AKI plus furosemide to keep it off their chest” isn’t a thing - commit to goal of wetter or drier.
(specialist use only eg. ⬆️Ca, ⬆️K)
Aug 18, 2019 • 20 tweets • 8 min read
To celebrate 1 yr of taking referrals as the renal registrar on-call, it’s time for some kidney-themed #tipsfornewdocs covering high K, AKI, “nephrotoxins”, medications, iv contrast, hypertension, & caring for kidney transplant & dialysis patients. #nephpearls (thread)
⬆️K - Renal #tipsfornewdocs 1/18
✅ Insulin-dextrose is not benign (⬇️BM risk) & does not get rid of K (only hides it), therefore rather than give round after round do phone us for help!
✅ Repeat ECG, re-bolus calcium gluconate if persistent changes
✅ Salbutamol dose = 10-20mg