
CUTANEOUS LUPUS – a #tweetorial/#medthread!!
We all learn about Systemic Lupus Erythematosus (SLE) in medical school, but did you know there are multiple forms #lupus can take in the #skin?
#Meded #FOAMed #dermtwitter #medtwitter #rheumtwitter #dermatologia pc: @dermnetnz
1/
We all learn about Systemic Lupus Erythematosus (SLE) in medical school, but did you know there are multiple forms #lupus can take in the #skin?
#Meded #FOAMed #dermtwitter #medtwitter #rheumtwitter #dermatologia pc: @dermnetnz
1/
It wasn’t until #dermatology residency I learned about all the subtypes of cutaneous lupus (CLE)! I thought it was all just one disease: SLE. But in reality there are many forms of CLE, each with its own implications on systemic involvement and effect on the patient.
2/
2/
Let’s start with the 3 subtypes:
Acute, Subacute, and Chronic Cutaneous Lupus Erythematosus (ACLE, SCLE, CCLE). CCLE is aka Discoid.
Each subtype "overlaps" with SLE in a different way.
Eg: ACLE overlaps completely with SLE, so they all have SLE! 👇
onlinelibrary.wiley.com/doi/abs/10.111…
3/
Acute, Subacute, and Chronic Cutaneous Lupus Erythematosus (ACLE, SCLE, CCLE). CCLE is aka Discoid.
Each subtype "overlaps" with SLE in a different way.
Eg: ACLE overlaps completely with SLE, so they all have SLE! 👇
onlinelibrary.wiley.com/doi/abs/10.111…
3/

ACLE is the typical “malar rash” we all learn in #medschool. Patients with ACLE theoretically all have SLE!
Main items on the ddx for ACLE are things like rosacea, seborrheic dermatitis, and other facial rashes. To differentiate, ACLE spares which of the following areas?
4/
Main items on the ddx for ACLE are things like rosacea, seborrheic dermatitis, and other facial rashes. To differentiate, ACLE spares which of the following areas?
4/
The nasolabial fold (NLF) is classically spared in ACLE, whereas seborrheic dermatitis and rosacea can involve this area! Patients with ACLE, given their high likelihood of having SLE, should probably be seeing our #rheumatology colleagues as well!
5/
5/


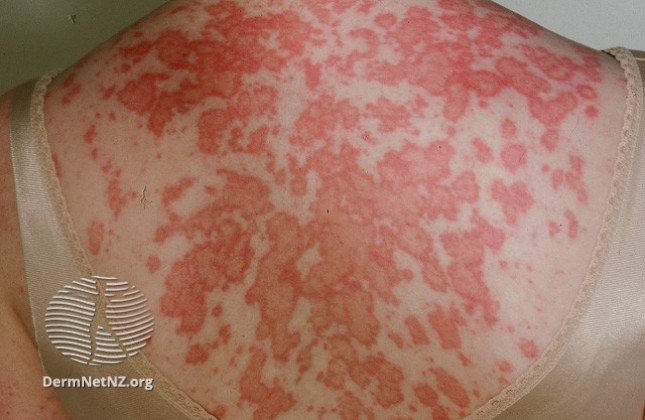
SCLE looks like a scaly eruption that is photodistributed. The overlap with SLE is smaller than ACLE, so some patients can get SCLE only (without systemic involvement).
There is a form of drug-induced SCLE that is Ro-positive (different from drug induced SLE).
6/
There is a form of drug-induced SCLE that is Ro-positive (different from drug induced SLE).
6/

CCLE (discoid lupus) is a scarring process that usually is on the head and neck. This is ideally found early so as to prevent the scarring process. An alopecia is common, and on exam, it classically involves the conchal bowls. Overlap with SLE is low, but still possible.
7/
7/


Brief interlude for a midway recap:
-ACLE is the malar rash. This spares the NLF.
-SCLE is scaly and photo distributed, can be drug induced.
-CCLE is on head and neck, look at conchal bowls and for alopecia.
-Each subtype has a different risk of having SLE.
8/
-ACLE is the malar rash. This spares the NLF.
-SCLE is scaly and photo distributed, can be drug induced.
-CCLE is on head and neck, look at conchal bowls and for alopecia.
-Each subtype has a different risk of having SLE.
8/
Bullous lupus is Ab-mediated and usually starts on dorsal hands. The bullae are tense (because the split happens at the BMZ). The ddx for this includes porphyria cutanea tarda and epidermolysis bullosa acquisita. This responds well to dapsone!
(Pic is EBA, but similar look!)
9/
(Pic is EBA, but similar look!)
9/

Lupus panniculitis, since deep, usually doesn’t have surface change, but patients will have deep inflammatory processes that can be painful, that then become atrophic over time. Main differential includes all other panniculitic processes like erythema nodosum!
10/
10/


And one for our #pediatric crowd. Neonatal LE presents with annular scaly plaques. These babies need EKGs to rule out heart block (+/- cardiomyopathy). Their mothers are the ones that have SLE that passed along an auto-antibody through the placenta. Which Ab was it?
11/
11/
Anti-Ro is the reason for neonatal LE, which also comes with risk of anemia, thrombocytopenia and hepatobiliary disease. Usually, the NLE resolves with time, but the sequelae (eg: heart block) can be permanent. Check out the photo of the characteristic rash!
12/
12/

And one note to say that SLE can also involve the skin in other ways. These include oral ulcers, rash on the dorsal hands (especially around nailfolds, and not limited to knuckles like in dermatomyositis), and dilated nailfold capillary loops.
13/
13/


The work up of CLE types can include a biopsy, but often the physical exam is enough to make a clinical diagnosis. A good history is all you need with some select auto-antibody testing. I try to avoid a huge laundry list of labs to send, but will keep SLICC in mind.
14/
14/

One last tiny point. #Dermatologists like to confuse people, so these two things are NOT lupus:
1 - Lupus Pernio (pic 1 - actually sarcoid)
2 - Lupus Vulgaris (pic 2 - actually TB)
As opposed to (pic3) "pernio," which can be associated w/lupus, despite not having the name.
15/
1 - Lupus Pernio (pic 1 - actually sarcoid)
2 - Lupus Vulgaris (pic 2 - actually TB)
As opposed to (pic3) "pernio," which can be associated w/lupus, despite not having the name.
15/



Summary:
-Many different forms of CLE, each with their own implications.
-Early diagnosis can help prevent permanent effects.
-Good history and select lab testing can help with diagnosis. Biopsy helps in some cases.
-Collaboration between #derm and #rheum are crucial!
16/
-Many different forms of CLE, each with their own implications.
-Early diagnosis can help prevent permanent effects.
-Good history and select lab testing can help with diagnosis. Biopsy helps in some cases.
-Collaboration between #derm and #rheum are crucial!
16/
Thanks all for joining me. I didn’t comment on #dermpath if a biopsy is taken, since we have such an active #dermpathtwitter group here, I’ll let them fill in the details. Also, hope this helps some of you out in #medstudenttwitter too! Until next time!
17/17
17/17
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















{kind=link}