1/N thread on Nat’l #COVID19 Clinical Rounds Apr 7 relevant images at END of thread
2/N Mark Cardi Emory U:Outcome vary on patient mix, location and resources
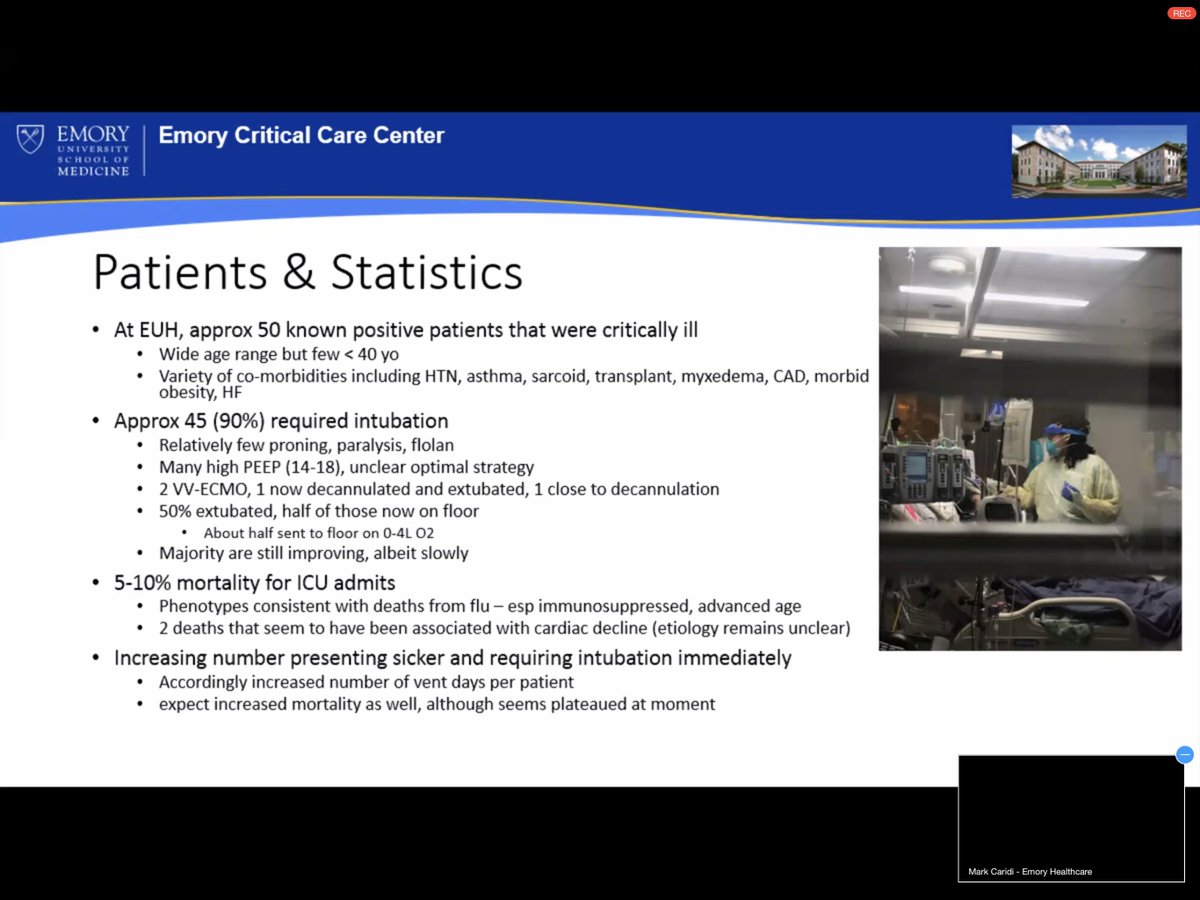
3/N Rapid moving, but plateaus with rapid transition
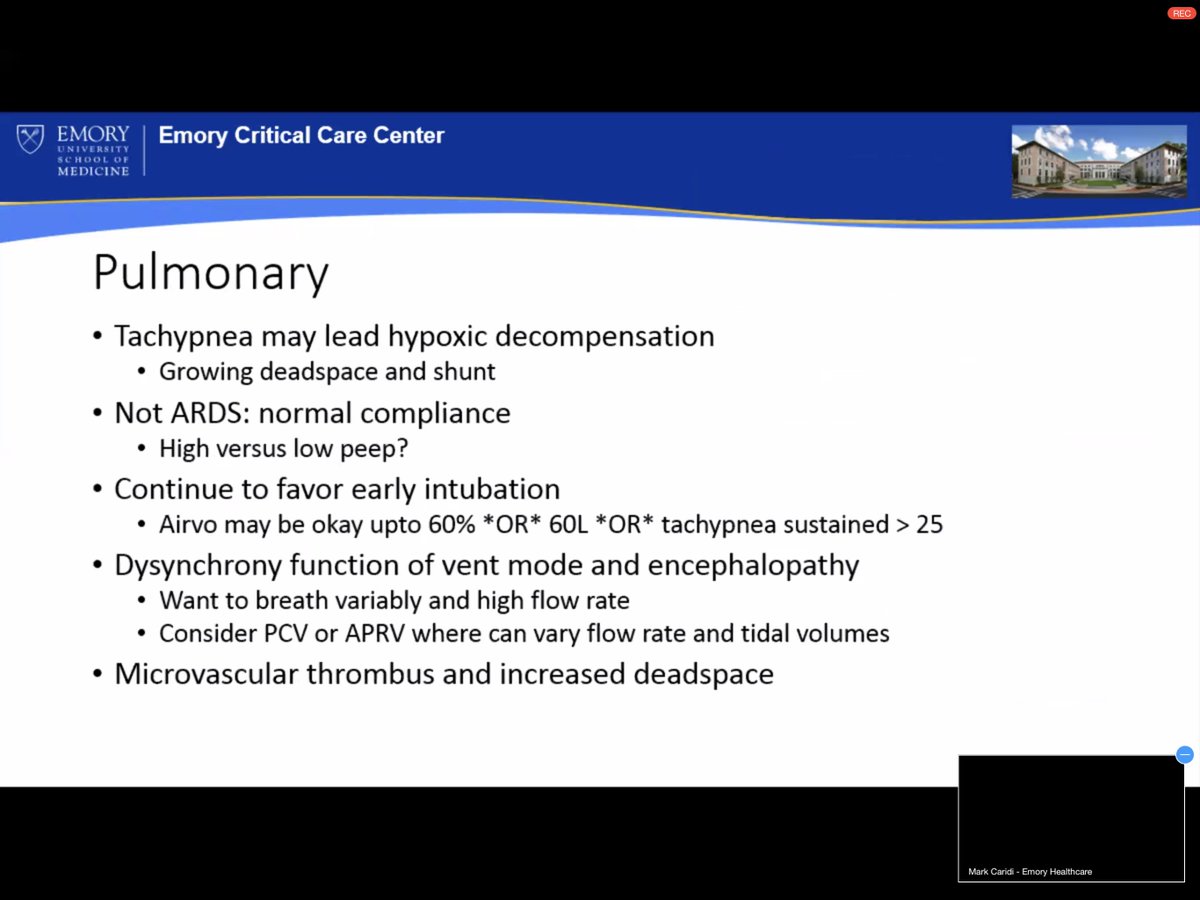
Tachypnea early warning
90%of ICU require intubation
5-10% of ICU mortality
Tachypnea early warning
90%of ICU require intubation
5-10% of ICU mortality
4/N cardiac death of unclear cause
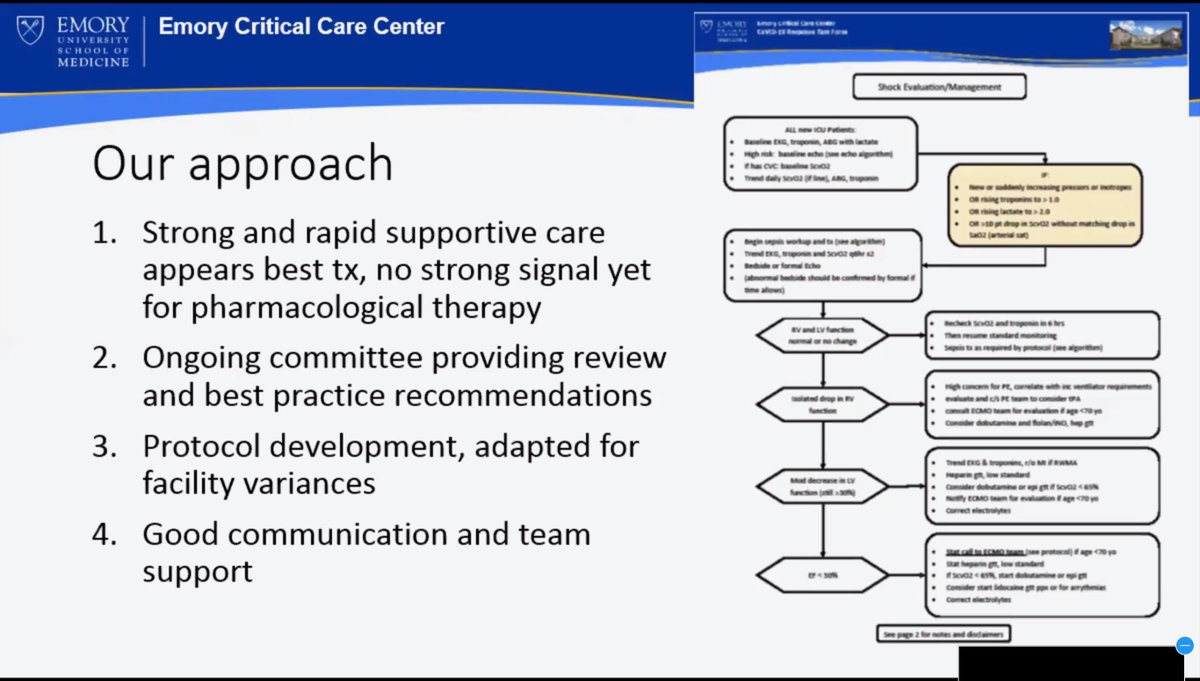
no strong ‘signal’ in pharma therapy
COVID19 isn’t normal ARDS
some real struggles with finding right ventilation approach
no strong ‘signal’ in pharma therapy
COVID19 isn’t normal ARDS
some real struggles with finding right ventilation approach
5/N Hypercoagulability
clotting lines, pulmonary deadspace
connected to heart issues, perhaps sudden death
Supportive care #1 therapy
clotting lines, pulmonary deadspace
connected to heart issues, perhaps sudden death
Supportive care #1 therapy
6/N Avoiding BiPAP
diabetes + hypertension
two forms of ECMO, one supplement heart & lungs, other approach just lung function
two forms of ECMO, one supplement heart & lungs, other approach just lung function
9/N now using a hybrid ECMO approach
note: this is very sparsely resourced device/approach
~160 COVID cases treated with ECMO
patient recovering with ECMO
IL-6 Receptor Antagonist lessened inflammation
Moving this forward in using this treatment
note: this is very sparsely resourced device/approach
~160 COVID cases treated with ECMO
patient recovering with ECMO
IL-6 Receptor Antagonist lessened inflammation
Moving this forward in using this treatment
10/N Paul Biddinger, MD Mass General
ECMO has been life saving for the small fraction that have needed it
ECMO has been life saving for the small fraction that have needed it
11/N Mukherjee Vikramjit, MD Bellevue Hospital NYC, NYU School of Med:
Need for renal replacement therapy big unanticipated demand, creating shortages
Need for renal replacement therapy big unanticipated demand, creating shortages
12/N ? Levels of sedation for vent synchronization
?Blocking cytokine storm
?Anticoagulation
?End of Life Care
?Blocking cytokine storm
?Anticoagulation
?End of Life Care
13/N seen massive pulmonary embolisms
sometimes GI bleeds from anticoagulant therapy
sometimes GI bleeds from anticoagulant therapy
14/N Clinical care is at best supportive; no clear therapy direction
building teams for Trach, Proning, Palliative, Procedures and Renal replacement
building teams for Trach, Proning, Palliative, Procedures and Renal replacement
15/N Morale will take a hit as health care worker getting sick; and 20-25% mortality rate.
emphasize smallest wins; recognize burnout. If you’re aren’t at 100% patients suffer
emphasize smallest wins; recognize burnout. If you’re aren’t at 100% patients suffer
16/N flying without much data; let go of patients and non-intensivists work with patients - Standardize care
17/N Account for space, AND STAFF
Must plan for staff getting sick
Must plan for staff getting sick
18/N errata: Mark *Caridi* at Emory
takeaways— still many unanswered questions, therapeutic paths are unclear, driven by adverse events
takeaways— still many unanswered questions, therapeutic paths are unclear, driven by adverse events
19/N smaller centers need to learn how to do things they avoid doing now
20/N Paul Biddinger,MD Mass General need huge menu of options staff support, mindfulness options, sharing good stories
22/n 
23/N
24/N