
*Caution, non-peer-reviewed preprint* Posted on @medrxivpreprint is our 1st look at characteristics and outcomes of #COVID19 patients @nyulangone. Will update for publication. But, here is early data in response to many ?s. @PetrilliMD @jones_prof /1 medrxiv.org/content/10.110… 
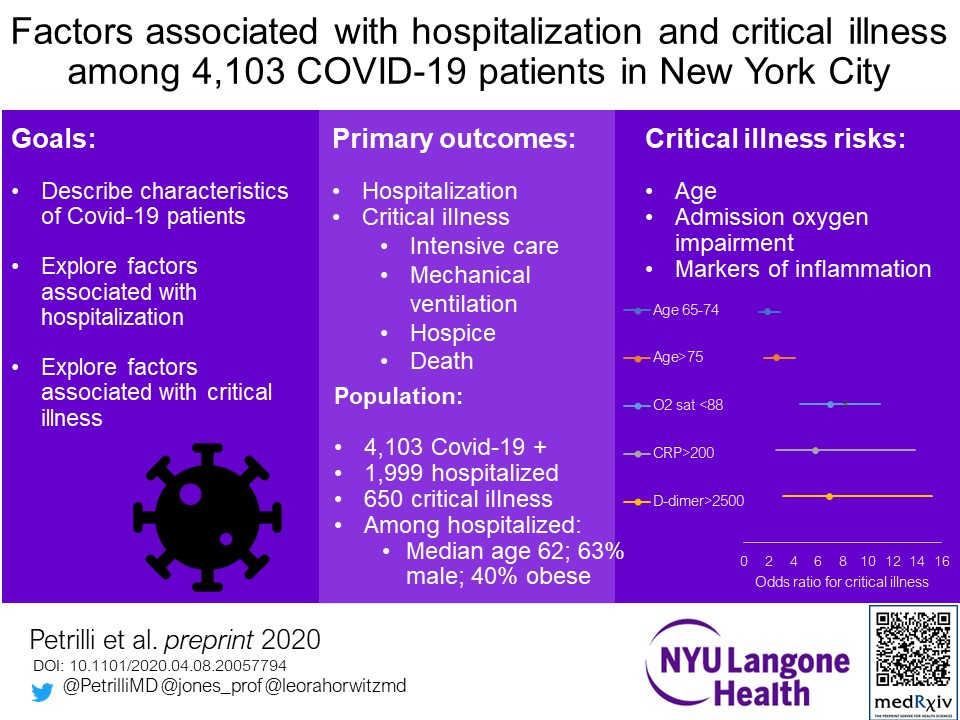
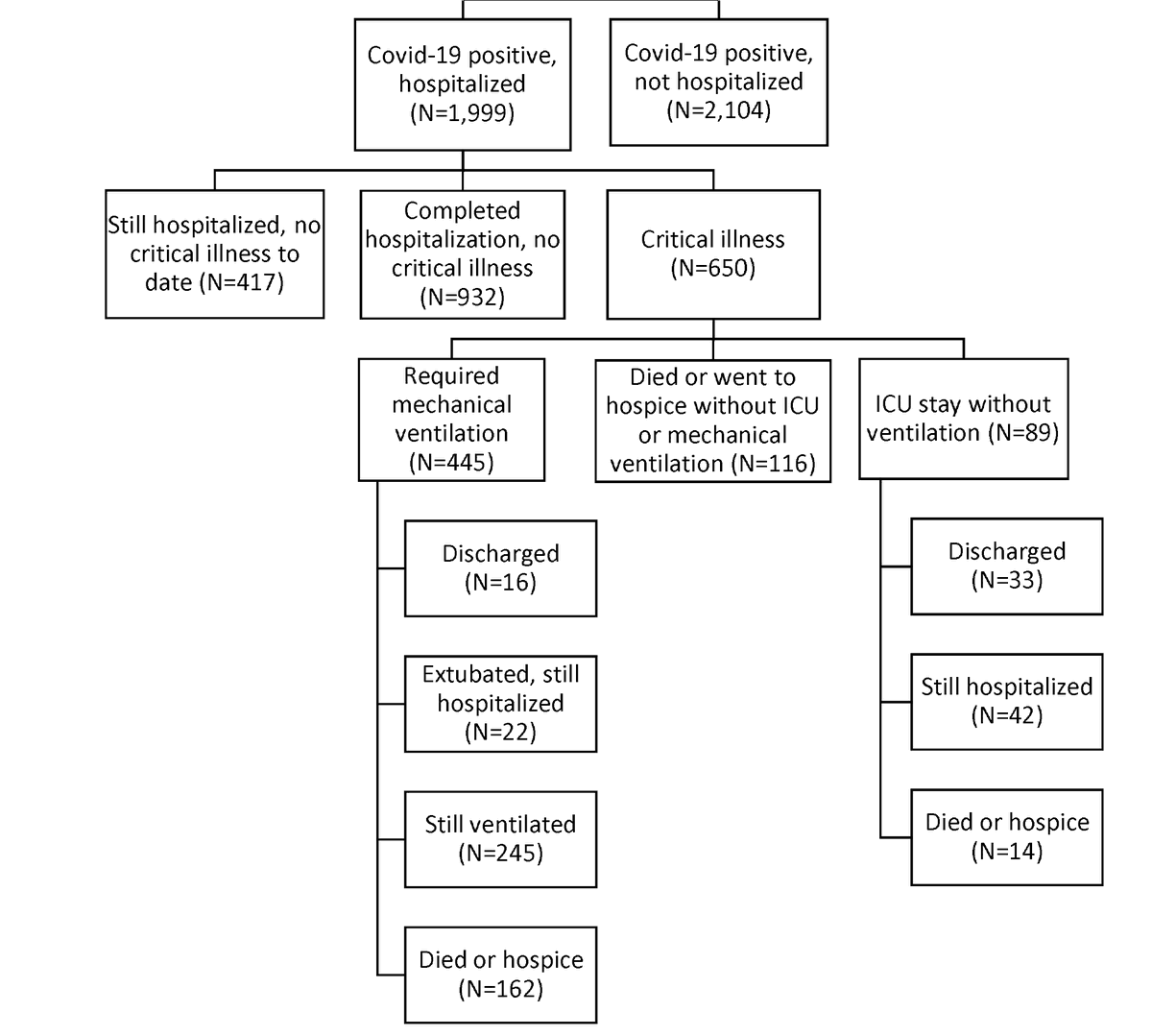
There is so much to unpack in these results. Will point out a few highlights. First, who is in the sample? 4,103 patients testing positive, of whom 1,999 hospitalized; 650 of those any of ICU/intubated/hospice/deceased ("critical illness"). This is largest US series I know of.
Overall outcomes (see figure): 32% crit illness, 46% discharged without critical illness, 21% still hospitalized without crit illness. Among crit illness, 45% mortality/hospice to date (36% of intubated), 9% extubated +/- discharged, 44% still hospitalized (median 11d follow up).
Hospitalized pts more often male (63% vs 39%), cardiac disease (45% vs 16%), diabetes (25% vs 5%), obese (40% vs 15%). *Once hospitalized, though, less difference critical illness vs not*: male (68% vs 60%), CV dis (47% vs 42%), diabetes (27% vs 23%), obesity (40% vs 41%).
In multivariable modeling, age is far and away strongest predictor of needing hospitalization (age 75+ odds ratio (OR) 67!; age 65-74 OR 11 vs age 19-44) with obesity next (BMI >40 OR 6.2; 30-40 OR 4.3 vs BMI <30); also HF (OR 4.3), CKD (OR 3.1).
(Note, though, that 54% hospitalized patients < age 65; 34% <55 years. Don't assume that because advanced age is such a huge risk factor that younger people don't get hospitalized.)
Male sex is still a risk for hospitalization even after adjustment: OR 2.8. Note what is not, though: hypertension (OR 1.2 not sig), COPD/asthma (OR 1.3, not sig), current/former smoking (OR 0.7). Don't understand the smoking results yet, looking more at this.
As for what makes someone likely to have critical illness when hospitalized? Evidence of inflammation on admission much stronger predictor than age/sex/comorbidities: CRP>200 OR 5.8; d-dimer >2,500 OR 6.9, plus of course whether already hypoxic (O2 sat <88 OR 7).
Age >75 still risk for critical illness even given labs (OR 2.6), but smoking, pulmonary disease still nothing there. Male sex does not confer additional risk for critical illness.
In this context we find it interesting that obesity is such a strong comorbidity risk given it is a hyperinflammatory state. #medtwitter: thoughts welcome as we refine for publication. Thanks to @venkmurthy @boback who have already provided Twitter peer review!
Adding co-author @WhiteCoatLuke, who has done more #COVID19 hospitalist time than virtually anyone else at our place.
Found some more coauthor handles! Credit also to @Cerf_MD @Francois1Fritz

